

A multidisciplinary approach to an unusual medical case of locally advanced gastric cancer: a case report
- PMID: 25619316
- PMCID: PMC4407615
- DOI: 10.1186/1752-1947-9-13
A multidisciplinary approach to an unusual medical case of locally advanced gastric cancer: a case report
Abstract
Introduction: Complete abdominal wall infiltration with neoplastic gastrocutaneous fistula is an unexpected and out of the ordinary presentation of locally advanced gastric cancer. It is very rare to encounter case reports presenting diffuse abdominal wall invasion, but a complete parietal destruction is an exceptional event.
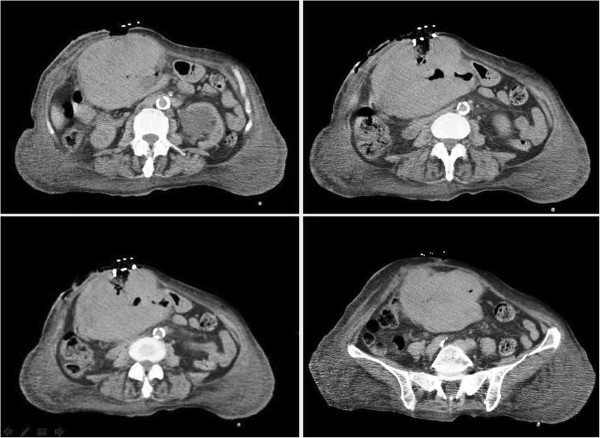
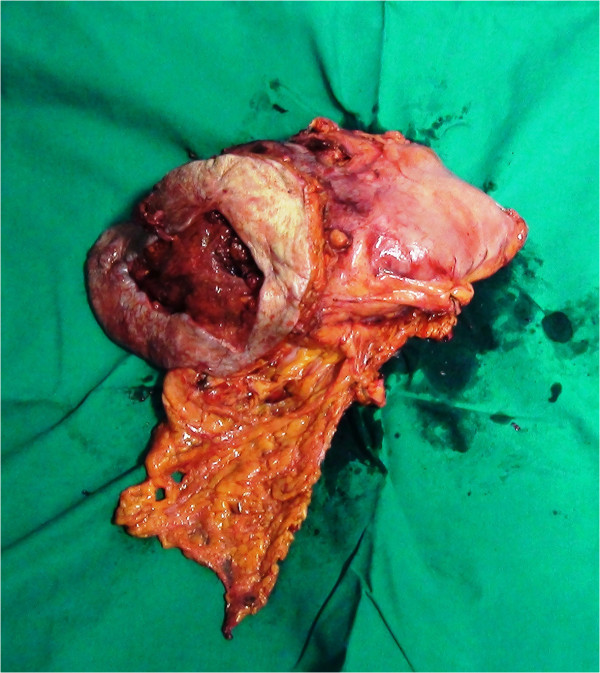
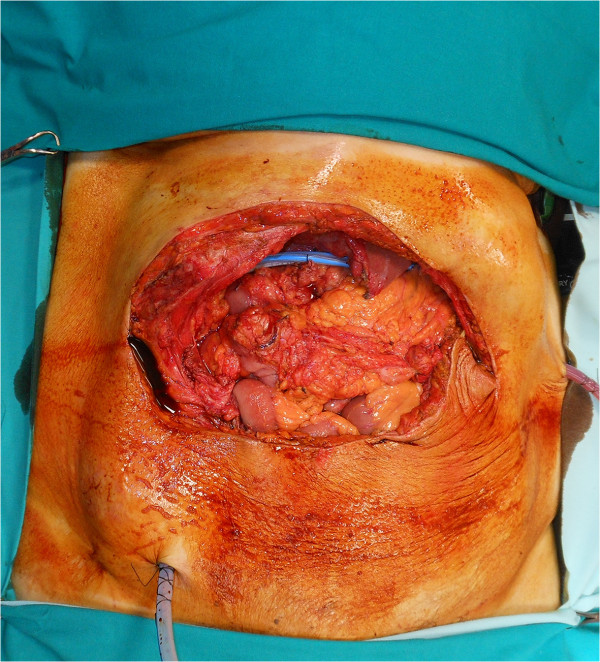
Case presentation: Here we describe the case of an 81-year-old Caucasian woman presenting a carcinoma perforating her anterior gastric wall and infiltrating all layers of her abdominal wall. The gastric tumor infiltrated her transverse mesocolon, the rectus abdominis muscles bilaterally and overran them anteriorly, causing a large parietal deficit and a complete external fistula. Treatment consisted of a complex surgical procedure requiring general and reconstructive surgery cooperation in order to perform an en bloc gastric resection including colon and abdominal wall, followed by a parietal reconstruction through positioning of prosthesis and reverse abdominoplasty.
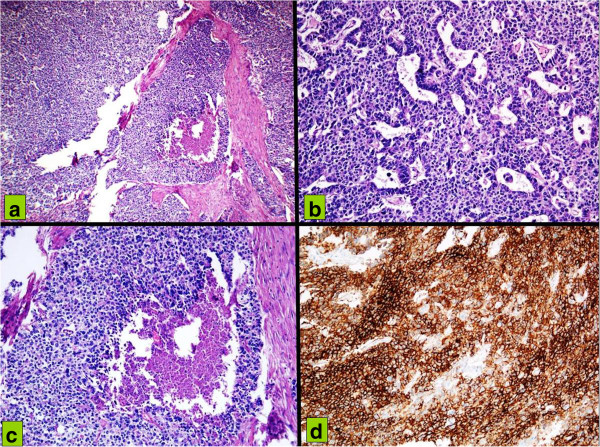
Conclusions: Clinical presentation, histology and therapeutic options are discussed. The importance of a multidisciplinary approach when encountering extremely rare clinical presentations is emphasized.
Figures


References
-
- Santangelo M, Vescio G, Sommella L, Battaglia M, Valente A, Sammarco G, Bossa F, Triggiani E. Extended total gastrectomy: indications in the 3rd millennium. Minerva Chir. 2001;56(1):1–6. - PubMed
-
- Tammaro V, Carlomagno N, Lombari P, Tedesco G, Renda A. Prognostic value of splenectomy and lymph-node dissection during gastric cancer resection. Chir Ital. 2006;58(2):163–170. - PubMed
-
- Feczko PJ, Collins DD, Mezwa DG. Metastatic disease involving the gastrointestinal tract. Radiol Clin North Am. 1993;31:1359–1373. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
