

Non-contact low-frequency ultrasound therapy compared with UK standard of care for venous leg ulcers: a single-centre, assessor-blinded, randomised controlled trial
- PMID: 25619411
- PMCID: PMC7949520
- DOI: 10.1111/iwj.12389
Non-contact low-frequency ultrasound therapy compared with UK standard of care for venous leg ulcers: a single-centre, assessor-blinded, randomised controlled trial
Abstract
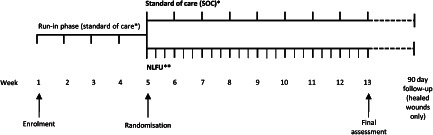
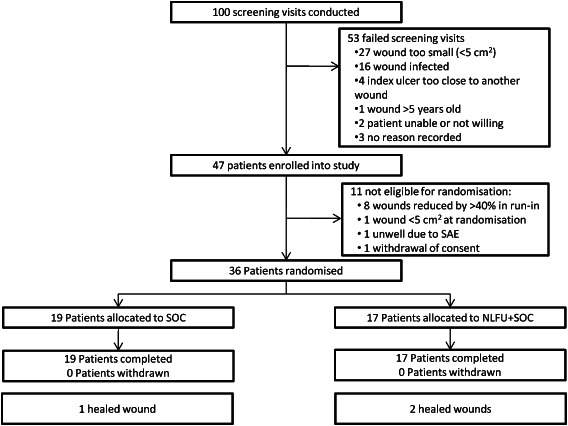
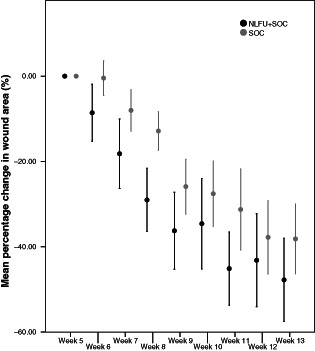
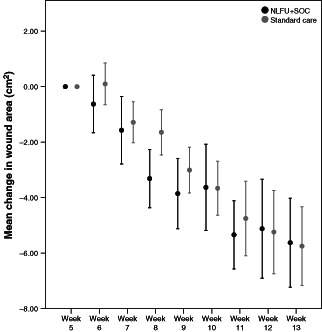
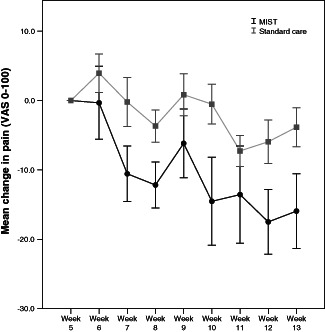
'Hard-to-heal' wounds are those which fail to heal with standard therapy in an orderly and timely manner and may warrant the use of advanced treatments such as non-contact low-frequency ultrasound (NLFU) therapy. This evaluator-blinded, single-site, randomised controlled trial, compared NLFU in addition to UK standard of care [SOC: (NLFU + SOC)] three times a week, with SOC alone at least once a week. Patients with chronic venous leg ulcers were eligible to participate. All 36 randomised patients completed treatment (17 NLFU + SOC, 19 SOC), and baseline demographics were comparable between groups. NLFU + SOC patients showed a -47% (SD: 38%) change in wound area; SOC, -39% (38%) change; and difference, -7·4% [95% confidence intervals (CIs) -33·4-18·6; P = 0·565]. The median number of infections per patient was two in both arms of the study and change in quality of life (QoL) scores was not significant (P = 0·490). NLFU + SOC patients reported a substantial mean (SD) reduction in pain score of -14·4 (14·9) points, SOC patients' pain scores reduced by -5·3 (14·8); the difference was -9·1 (P = 0·078). Results demonstrated the importance of high-quality wound care. Outcome measures favoured NLFU + SOC over SOC, but the differences were not statistically significant. A larger sample size and longer follow-up may reveal NLFU-related improvements not identified in this study.
Keywords: Compression; Quality of life; Ultrasound therapy; Venous leg ulcers; Wound healing.
© 2015 The Authors. International Wound Journal published by Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Figures
References
-
- Scottish Intercollegiate Guidelines Network . Management of chronic venous leg ulcers: a national clinical guideline (SIGN Guideline 120). Edinburgh: Scottish Intercollegiate Guidelines Network, 2010.
-
- Troxler M, Vowden K, Vowden P. Integrating adjunctive therapy into practice: the importance of recognising ‘hard‐to‐heal’ wounds. [WWW document]. URL http://www.worldwidewounds.com/2006/december/Troxler/Integrating-Adjunct... [accessed on 4 November 2014].
-
- Lazarus G, Valle MF, Malas M, Qazi U, Maruthur NM, Doggett D, Fawole OA, Bass EB, Zenilman J. Chronic venous leg ulcer treatment: future research needs. Wound Repair Regen 2014;22:34–42. - PubMed
-
- Graham ID, Harrison MB, Nelson EA, Lorimer K, Fisher A. Prevalence of lower‐limb ulceration: a systematic review of prevalence studies. Adv Skin Wound Care 2003;16:305–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
