

Cost-effectiveness of point-of-care C-reactive protein tests for respiratory tract infection in primary care in England
- PMID: 25620538
- PMCID: PMC4311066
- DOI: 10.1007/s12325-015-0180-x
Cost-effectiveness of point-of-care C-reactive protein tests for respiratory tract infection in primary care in England
Abstract
Introduction: Despite recommendations that general practitioners (GPs) delay antibiotic prescribing for respiratory tract infections (RTIs), antibiotic prescriptions in primary care in England increased by 4.1% from 2010 to 2013. C-reactive protein (CRP) point-of-care tests (POCT), for example, the Afinion™ Analyzer (Alere Ltd, Stockport, UK) device, are widely used in several countries in the European Union. Studies suggest that CRP POCT use, either alone or in combination with communication training, reduces antibiotic prescribing and improves quality of life for patients presenting with RTI symptoms. The aim of this study is to evaluate the cost-effectiveness of CRP POCT for RTIs in primary care in England over 3 years for three different strategies of care compared to standard practice.
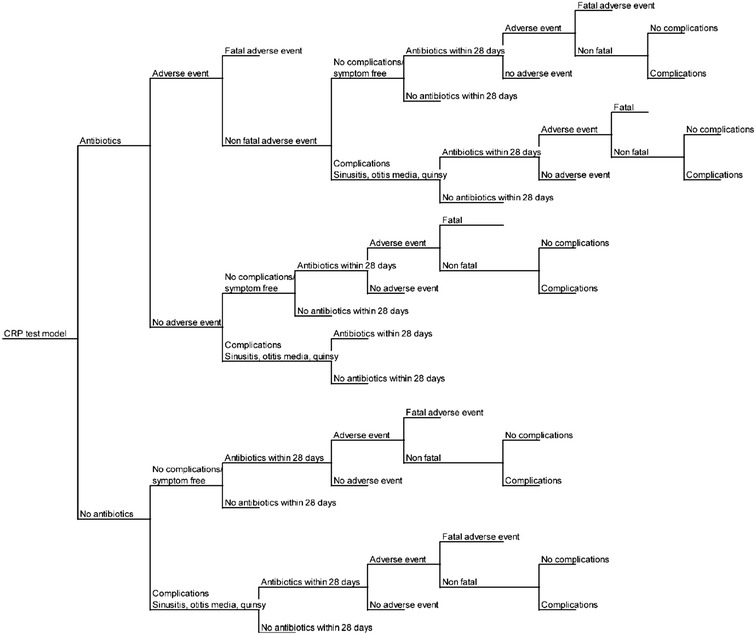
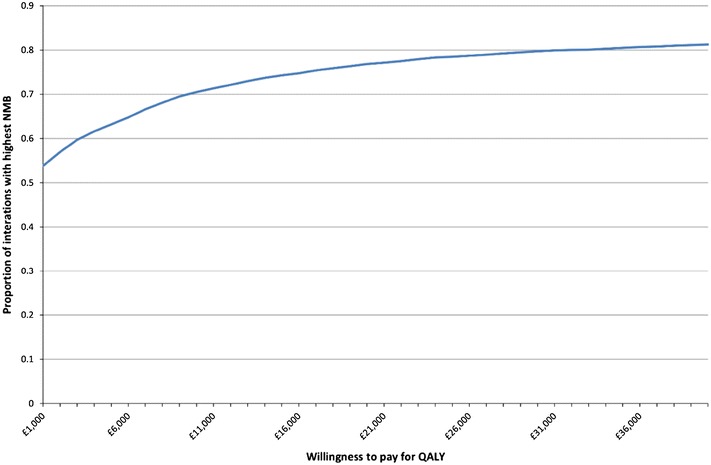
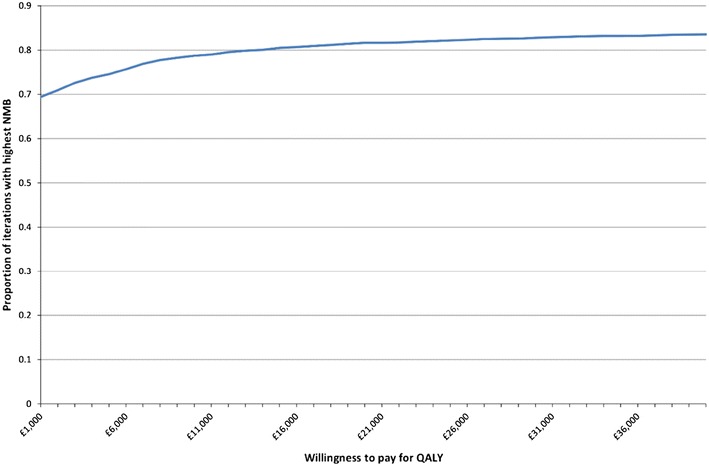
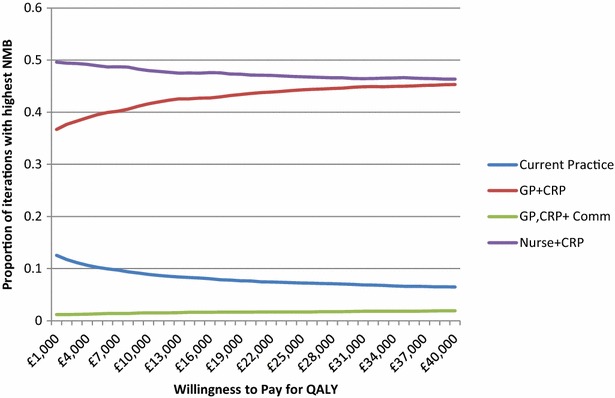
Methods: An economic evaluation was carried out to compare the costs and benefits of three different strategies of CRP testing (GP plus CRP; practice nurse plus CRP; and GP plus CRP and communication training) for patients with RTI symptoms as defined by National Institute for Health and Care Excellence guideline CG69, compared with current standard GP practice without CRP testing. Analysis consisted of a decision tree and Markov model to describe the quality-adjusted life years (QALYs) and cost per 100 patients, together with the number of antibiotic prescriptions and RTIs for each group.
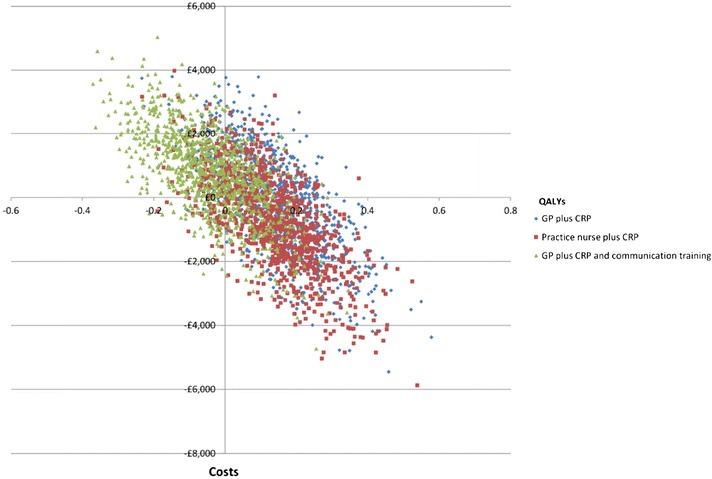
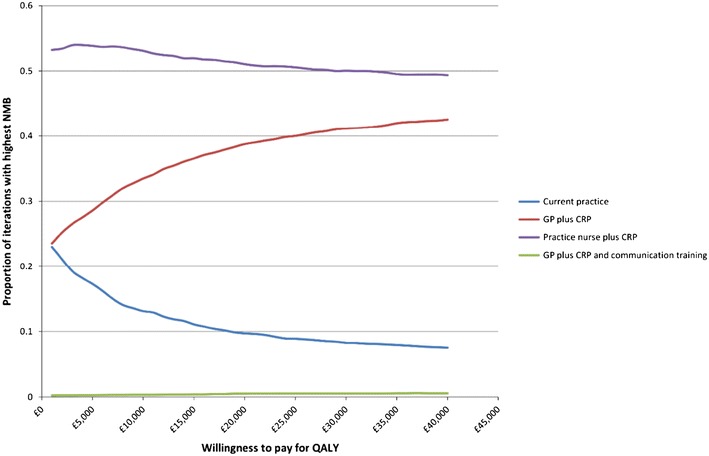
Results: Compared with current standard practice, the GP plus CRP and practice nurse plus CRP test strategies result in increased QALYs and reduced costs, while the GP plus CRP testing and communication training strategy is associated with increased costs and reduced QALYs. Additionally, all three CRP arms led to fewer antibiotic prescriptions and infections over 3 years.
Conclusion: The additional cost per patient of the CRP test is outweighed by the associated cost savings and QALY increment associated with a reduction in infections in the long term.
Figures
References
-
- Respiratory tract infections—antibiotic prescribing. NICE clinical guideline 69. NICE; London, UK; 2008. Available from: http://www.nice.org.uk/guidance/cg69/. Accessed 1 June 2014.
-
- Public Health England: English surveillance programme for antimicrobial utilisation and resistance (ESPAUR). Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil.... Accessed 1 June 2014.
-
- Department of Health and Department for Environment, Food & Rural Affairs: UK Five Year Antimicrobial Resistance Strategy 2013 to 2018. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/fil.... Accessed 1 June 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
