

Reconstructive surgery in advanced perioral non-melanoma skin cancer. Results in elderly patients
- PMID: 25621090
- PMCID: PMC4299704
- DOI: 10.3315/jdcr.2014.1184
Reconstructive surgery in advanced perioral non-melanoma skin cancer. Results in elderly patients
Abstract
Background: Nonmelanoma skin cancer (NMSC) of the perioral region is not uncommon. Basal cell carcinoma is predominant in the upper lip area and squamous cell carcinoma in the lower lip area. While smaller lesions can be treated by excision followed by primary closure larger defects after tumor surgery can be challenging.
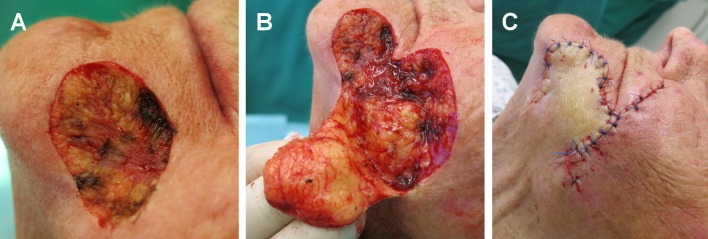
Objectives: Analysis of outcome after complete surgical excision with micrographical control of excision margins (delayed Mohs surgery) of large NMSC's of the perioral region (lips and chin).
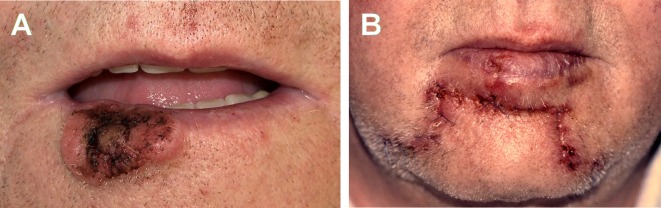
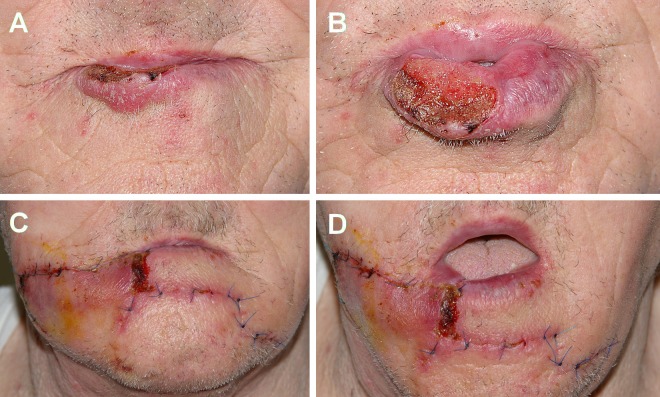
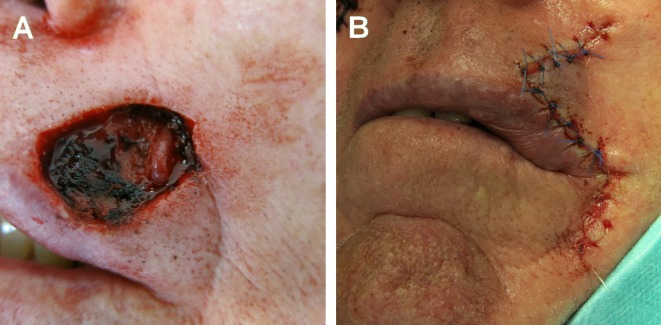
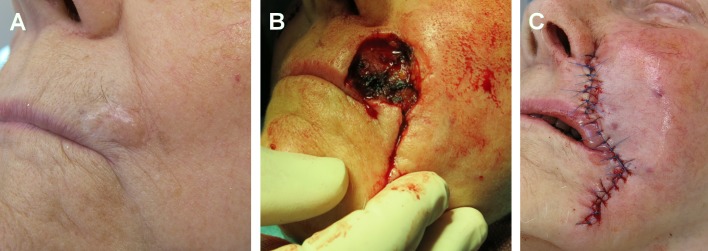
Patients and methods: This is a retrospective, single-center analysis of patients with defects after delayed Mohs surgery of ≥ 3 cm of the perioral region. The study included a total of 25 patients (4 women and 21 men) with a mean age of 83.7 years. Twenty patients were diagnosed with squamous cell carcinoma and five had basal cell carcinoma. The lower lip was affected in 19 patients, the upper lip in 4 patients and the chin in 2 patients. Tumor stage was either T1N0M0 or T2N0M0. The most common procedure for lower lip defect closure was staircase or modified staircase technique. Cheek advancement flaps were used for upper lip defect closure. Inferiorly based nasolabial rotational flap, cheek rotational flap and modified Webster flap were also employed. In one patient Webster flap and unilateral staircase technique were combined.
Results: In all patients the tumor was removed completely with preservation of function and aesthetics. No local recurrence was observed after a median follow-up of 4.9 years.
Conclusion: Perioral reconstruction after removal of large NMSC is a complex issue. The age group of over 70 years, frequently with comorbidities, requires a robust surgical technique with short operation times and tailored approaches for defect closure.
Keywords: advancement flaps; defect closure; perioral region; rotational flaps; skin cancer.
Figures


Similar articles
-
Lip Repair after Mohs Surgery for Squamous Cell Carcinoma by Bilateral Tissue Expanding Vermillion Myocutaneous Flap (Goldstein Technique Modified by Sawada).Open Access Maced J Med Sci. 2018 Jan 10;6(1):93-95. doi: 10.3889/oamjms.2018.034. eCollection 2018 Jan 25. Open Access Maced J Med Sci. 2018. PMID: 29483995 Free PMC article.
-
Characteristics of non-melanoma skin cancers of the cutaneous perioral and vermilion lip treated by Mohs micrographic surgery.J Eur Acad Dermatol Venereol. 2019 Feb;33(2):305-311. doi: 10.1111/jdv.15263. Epub 2018 Nov 6. J Eur Acad Dermatol Venereol. 2019. PMID: 30284728
-
Lower Lip Reconstruction Using the Karapandzic Flap Technique.Cureus. 2023 Dec 21;15(12):e50929. doi: 10.7759/cureus.50929. eCollection 2023 Dec. Cureus. 2023. PMID: 38249179 Free PMC article.
-
Reconstruction of Defects Involving the Lip and Chin.Facial Plast Surg Clin North Am. 2019 Feb;27(1):67-83. doi: 10.1016/j.fsc.2018.08.008. Facial Plast Surg Clin North Am. 2019. PMID: 30420074 Review.
-
Reconstruction of Mohs Defects of the Lips and Chin.Facial Plast Surg Clin North Am. 2017 Aug;25(3):427-442. doi: 10.1016/j.fsc.2017.03.012. Facial Plast Surg Clin North Am. 2017. PMID: 28676167 Review.
Cited by
-
Lip Repair after Mohs Surgery for Squamous Cell Carcinoma by Bilateral Tissue Expanding Vermillion Myocutaneous Flap (Goldstein Technique Modified by Sawada).Open Access Maced J Med Sci. 2018 Jan 10;6(1):93-95. doi: 10.3889/oamjms.2018.034. eCollection 2018 Jan 25. Open Access Maced J Med Sci. 2018. PMID: 29483995 Free PMC article.
-
Photoletter to the editor: Basal cell carcinoma on the vermilion lip.J Dermatol Case Rep. 2015 Mar 31;9(1):25-6. doi: 10.3315/jdcr.2015.1195. eCollection 2015 Mar 31. J Dermatol Case Rep. 2015. PMID: 25932061 Free PMC article.
References
-
- Dubas LE, Ingraffea A. Nonmelanoma skin cancer. Facial Plast Surg Clin North Am. 2013;21:43–53. - PubMed
-
- Akcam TM, Gubisch W, Unlu H. Nonmelanoma skin cancer of the head and neck: surgical treatment. Facial Plast Surg Clin North Am. 2012;20:455–471. - PubMed
-
- Eskiizmir G, Baker S, Cingi C. Nonmelanoma skin cancer of the head and neck: reconstruction. Facial Plast Surg Clin North Am. 2012;20:493–513. - PubMed
-
- Hauschild A, Breuninger H, Kaufmann R, Kortmann RD, Schwipper V, Werner J, Reifenberger J, Dirschka T, Garbe C. Short German guidelines: basal cell carcinoma. J Dtsch Dermatol Ges. 2008;6 (Suppl 1):S2–4. - PubMed
-
- Breuninger H, Bootz F, Hauschild A, Kortmann RD, Wolff K, Stockfleth E, Szeimies M, Rompel R, Garbe C. Short German guidelines: squamous cell carcinoma. J Dtsch Dermatol Ges. 2008;6 (Suppl 1):S5–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources