

Right ventricle in acute and chronic pulmonary embolism (2013 Grover Conference series)
- PMID: 25621151
- PMCID: PMC4278597
- DOI: 10.1086/676748
Right ventricle in acute and chronic pulmonary embolism (2013 Grover Conference series)
Abstract
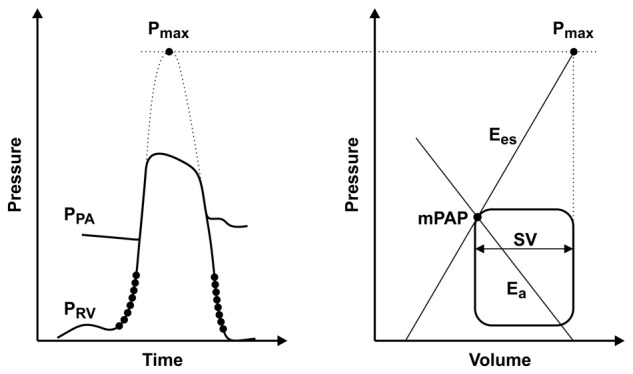
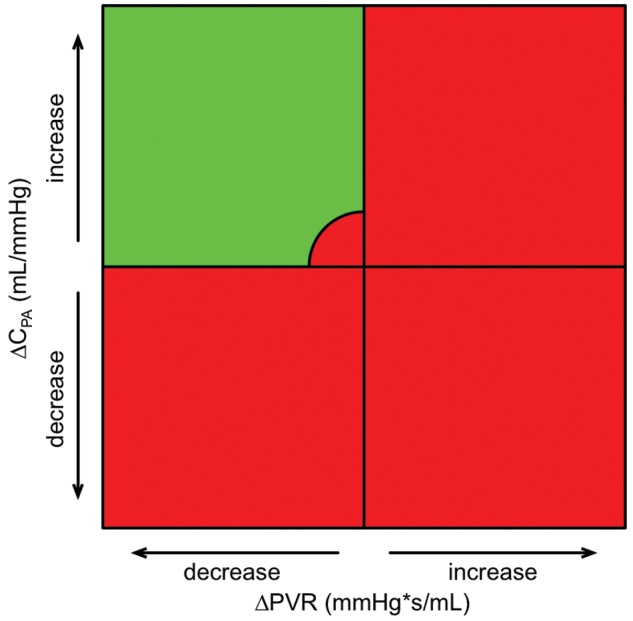
Venous thromboembolism (VTE) encompasses deep-vein thrombosis and pulmonary embolism (PE). It is the third-most-frequent cardiovascular disease, with an overall annual incidence of 1-2 per 1,000 population. Chronic thromboembolic pulmonary hypertension (CTEPH) is regarded as a late sequela of PE, with a reported incidence varying between 0.1% and 9.1% of those surviving acute VTE. Right ventricular (RV) function is dependent on afterload. The most precise technique to describe RV function is invasive assessment of the RV-to-pulmonary vascular coupling. However, assessments of RV afterload (i.e., steady and pulsatile flow components and their product, the RC-time) may be useful hemodynamic surrogates of coupling. RV load is different in acute and chronic PE. In acute PE, more than 60% occlusion of the cross-sectional area of the pulmonary artery within a short period of time leads to abrupt hemodynamic collapse. If the time of occlusion is limited to ∼15 seconds, significant decreases in fractional area change, tricuspid annulus systolic excursion, and RV free-wall deformation (strain) occur, with the latter showing significant postsystolic shortening. These changes have similarities to ischemic stunning, and they recover within minutes. In CTEPH, studies of pulmonary vascular resistance (PVR) and pulmonary arterial compliance demonstrated low RC-times that were further lowered after pulmonary endarterectomy (PEA). Immediate postoperative PVR was the only predictor of long-term survival/freedom from lung transplantation, suggesting that the effect of PEA on opening vascular territories to flow outweighs its effect on proximal stiffness. This review summarizes the current knowledge on vascular and intrinsic RV adaptation to VTE, including CTEPH, and the role of imaging.
Keywords: hemodynamics; pulmonary embolism; pulmonary heart disease; right ventricle.
Figures
Similar articles
-
Pathophysiology of right ventricular failure in acute pulmonary embolism and chronic thromboembolic pulmonary hypertension: a pictorial essay for the interventional radiologist.Insights Imaging. 2019 Feb 13;10(1):18. doi: 10.1186/s13244-019-0695-9. Insights Imaging. 2019. PMID: 30758687 Free PMC article. Review.
-
Long-term changes of resting and exercise right ventricular systolic performance in patients with chronic thromboembolic pulmonary hypertension following pulmonary thromboendarterectomy - A two-dimensional and three-dimensional echocardiographic study.Echocardiography. 2019 Sep;36(9):1656-1665. doi: 10.1111/echo.14456. Epub 2019 Aug 19. Echocardiography. 2019. PMID: 31424115
-
Utility of right ventricular Tei index in the noninvasive evaluation of chronic thromboembolic pulmonary hypertension before and after pulmonary thromboendarterectomy.JACC Cardiovasc Imaging. 2009 Feb;2(2):143-9. doi: 10.1016/j.jcmg.2008.10.012. JACC Cardiovasc Imaging. 2009. PMID: 19356547
-
Right ventricular strain before and after pulmonary thromboendarterectomy in patients with chronic thromboembolic pulmonary hypertension.Echocardiography. 2015 Jul;32(7):1115-21. doi: 10.1111/echo.12812. Epub 2014 Oct 18. Echocardiography. 2015. PMID: 25327878
-
Assessment of right ventricular systolic function by tissue Doppler echocardiography.Dan Med J. 2012 Mar;59(3):B4409. Dan Med J. 2012. PMID: 22381093 Review.
Cited by
-
Central versus Peripheral CTEPH-Clinical and Hemodynamic Specifications.Medicina (Kaunas). 2022 Oct 27;58(11):1538. doi: 10.3390/medicina58111538. Medicina (Kaunas). 2022. PMID: 36363494 Free PMC article.
-
Management of High-Risk Pulmonary Embolism: What Is the Place of Extracorporeal Membrane Oxygenation?J Clin Med. 2022 Aug 13;11(16):4734. doi: 10.3390/jcm11164734. J Clin Med. 2022. PMID: 36012973 Free PMC article. Review.
-
Saddle pulmonary embolism: right ventricular strain an indicator for early surgical approach.Oxf Med Case Reports. 2016 Jun 1;2016(6):130-4. doi: 10.1093/omcr/omw045. eCollection 2016 Jan. Oxf Med Case Reports. 2016. PMID: 27274856 Free PMC article.
-
Effect of Percutaneous Suction Thromboembolectomy on Improved Right Ventricular Function.Tex Heart Inst J. 2019 Apr 1;46(2):115-119. doi: 10.14503/THIJ-17-6551. eCollection 2019 Apr. Tex Heart Inst J. 2019. PMID: 31236075 Free PMC article.
-
Clinical and hemodynamic features of acute pulmonary embolism patients diagnosed in cold weather predicts adverse clinical outcome.Front Cardiovasc Med. 2022 Nov 10;9:1055926. doi: 10.3389/fcvm.2022.1055926. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36440035 Free PMC article.
References
-
- Riedel M, Stanek V, Widimsky J, Prerovsky I. Longterm follow-up of patients with pulmonary thromboembolism: late prognosis and evolution of hemodynamic and respiratory data. Chest 1982;81(2):151–158. - PubMed
-
- Lankhaar J-W, Westerhof N, Faes TJ, Marques KMJ, Marcus JT, Postmus PE, Vonk-Noordegraaf A. Quantification of right ventricular afterload in patients with and without pulmonary hypertension. Am J Physiol Heart Circ Physiol 2006;291(4):H1731–H1737. - PubMed
-
- Bonderman D, Martischnig AM, Vonbank K, Nikfardjam M, Meyer B, Heinz G, Klepetko W, Naeije R, Lang IM. Right ventricular load at exercise is a cause of persistent exercise limitation in patients with normal resting pulmonary vascular resistance after pulmonary endarterectomy. Chest 2011;139(1):122–127. - PubMed
-
- Lankhaar JW, Westerhof N, Faes TJ, Gan CT-J, Marques KM, Boonstra A, van den Berg FG, Postmus PE, Vonk-Noordegraaf A. Pulmonary vascular resistance and compliance stay inversely related during treatment of pulmonary hypertension. Eur Heart J 2008;29(13):1688–1695. - PubMed
-
- Mahapatra S, Nishimura RA, Sorajja P, Cha S, McGoon MD. Relationship of pulmonary arterial capacitance and mortality in idiopathic pulmonary arterial hypertension. J Am Coll Cardiol 2006;47(4):799–803. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
