

Biomechanics of the right ventricle in health and disease (2013 Grover Conference series)
- PMID: 25621153
- PMCID: PMC4278599
- DOI: 10.1086/677354
Biomechanics of the right ventricle in health and disease (2013 Grover Conference series)
Abstract
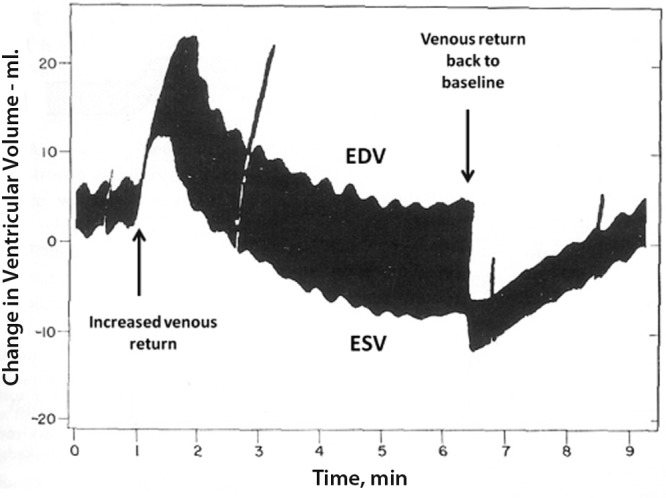
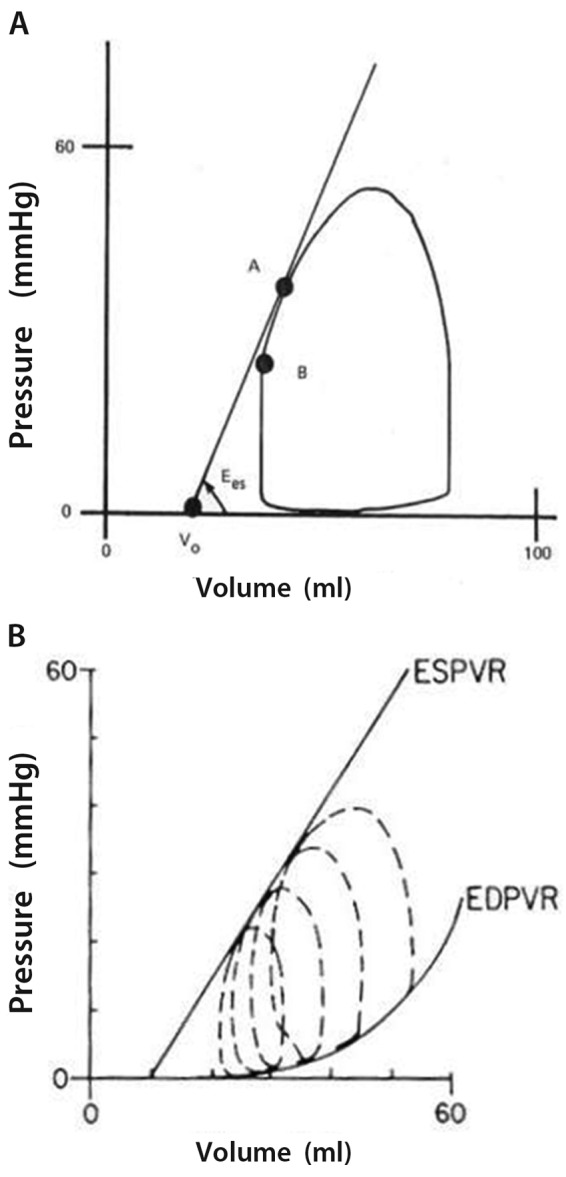
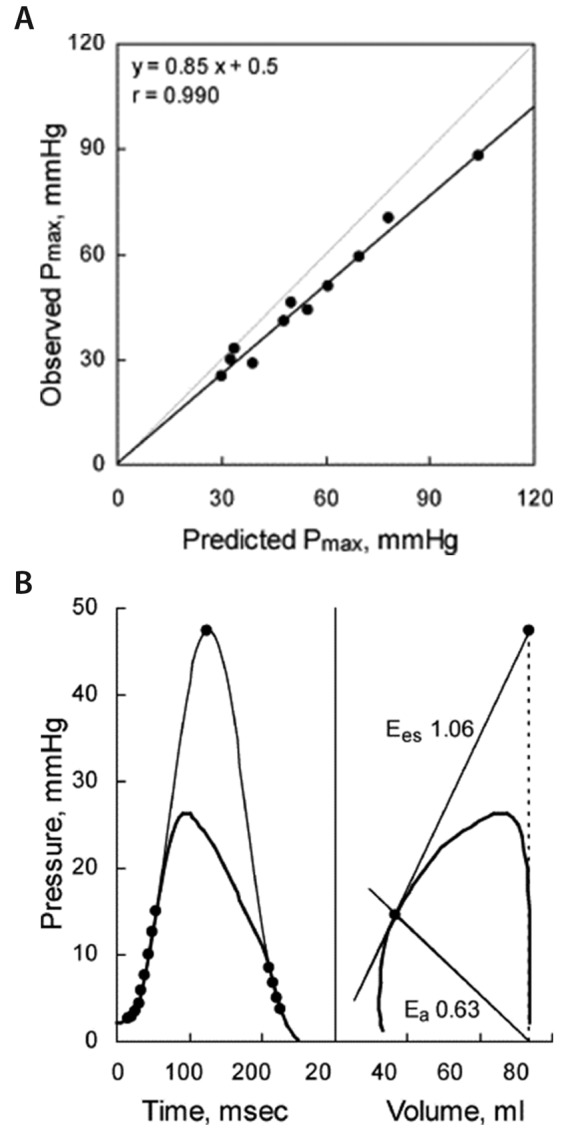
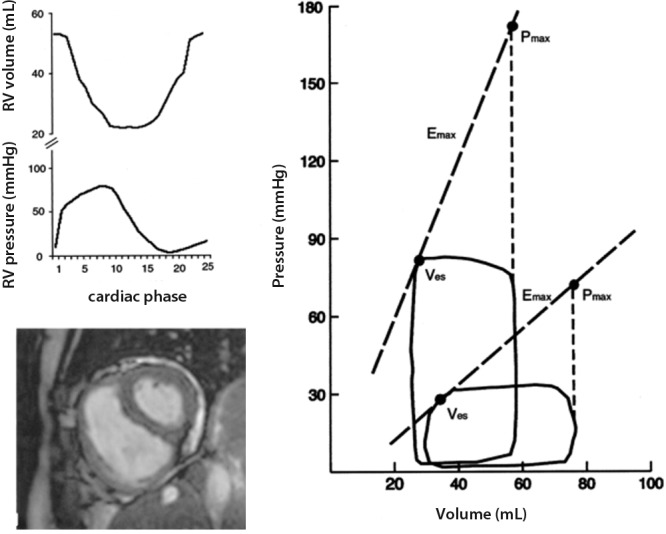
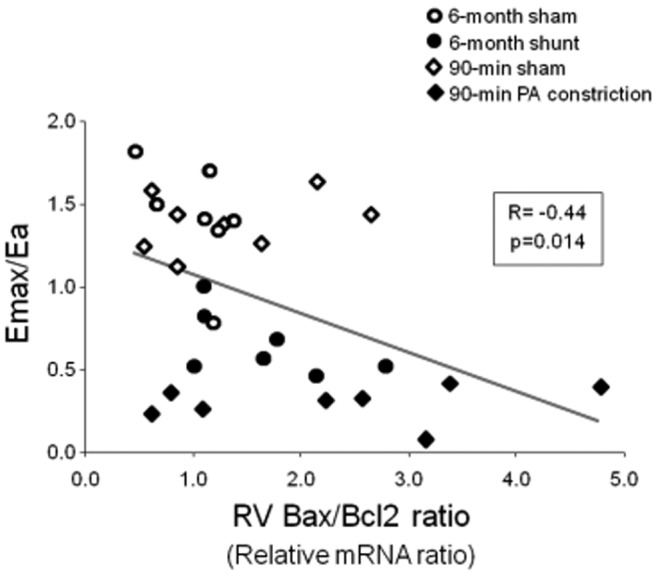
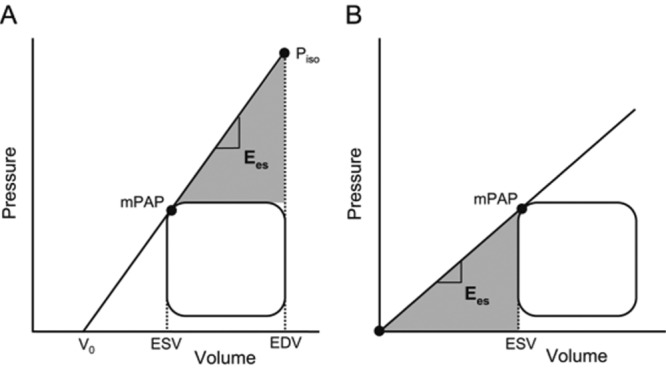
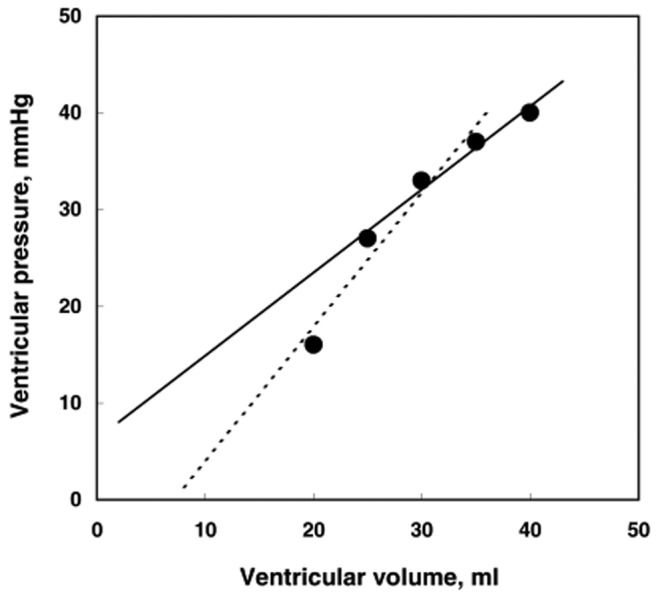
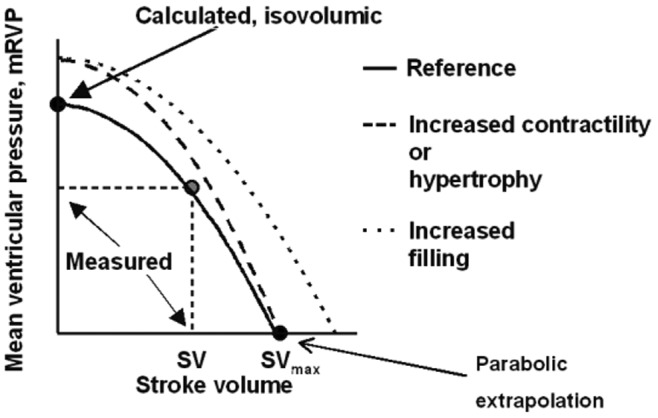
Right ventricular (RV) function is a major determinant of the symptomatology and outcome in pulmonary hypertension. The normal RV is a thin-walled flow generator able to accommodate large changes in venous return but unable to maintain flow output in the presence of a brisk increase in pulmonary artery pressure. The RV chronically exposed to pulmonary hypertension undergoes hypertrophic changes and an increase in contractility, allowing for preserved flow output in response to peripheral demand. Failure of systolic function adaptation (homeometric adaptation, described by Anrep's law of the heart) results in increased dimensions (heterometric adaptation; Starling's law of the heart), with a negative effect on diastolic ventricular interactions, limitation of exercise capacity, and vascular congestion. Ventricular function is described by pressure-volume relationships. The gold standard of systolic function is maximum elastance (E max), or the maximal value of the ratio of pressure to volume. This value is not immediately sensitive to changes in loading conditions. The gold standard of afterload is arterial elastance (E a), defined by the ratio of pressure at E max to stroke volume. The optimal coupling of ventricular function to the arterial circulation occurs at an E max/E a ratio between 1.5 and 2. Patients with severe pulmonary hypertension present with an increased E max, a trend toward decreased E max/E a, and increased RV dimensions, along with progression of the pulmonary vascular disease, systemic factors, and left ventricular function. The molecular mechanisms of RV systolic failure are currently being investigated. It is important to refer biological findings to sound measurements of function. Surrogates for E max and E a are being developed through bedside imaging techniques.
Keywords: afterload; arterial elastance; end-systolic elastance; maximum elastance; preload; pulmonary hypertension; right ventricle.
Figures
References
-
- Reeves JT, Groves BM, Turkevich D, Morrison DA, Trapp JA. Right ventricular function in pulmonary hypertension. In: Weir EK and Reeves JT, eds. Pulmonary vascular physiology and physiopathology. New York: Dekker, 1989:325–351.
-
- Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Meldrum DR, Dupuis J, et al. Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation 2006;114(17):1883–1891. - PubMed
-
- West JB. Role of the fragility of the pulmonary blood-gas barrier in the evolution of the pulmonary circulation. Am J Physiol Regul Integr Comp Physiol 2013;304(3):R171–R176. - PubMed
-
- Starr I, Jeffers WA, Meade RH. The absence of conspicuous increments of venous pressure after severe damage to the right ventricle of the dog, with a discussion of the relation between clinical congestive heart failure and heart disease. Am Heart J 1943;26(3):291–301.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
