

Physician attitudes toward palliative care for patients with pulmonary arterial hypertension: results of a cross-sectional survey
- PMID: 25621164
- PMCID: PMC4278610
- DOI: 10.1086/677365
Physician attitudes toward palliative care for patients with pulmonary arterial hypertension: results of a cross-sectional survey
Abstract
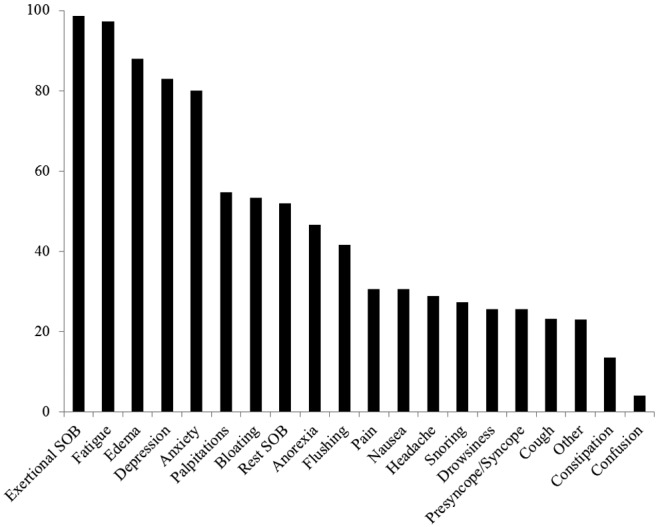
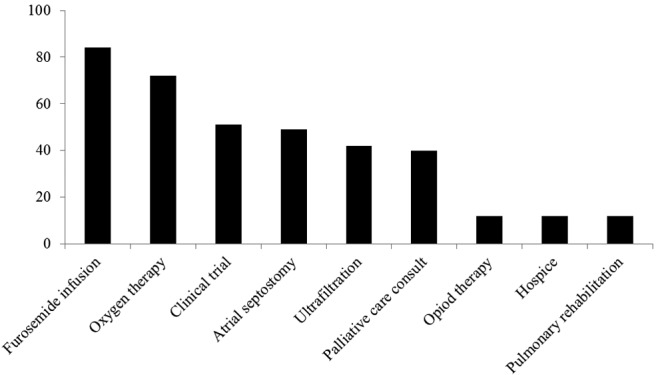
Pulmonary arterial hypertension (PAH) is a chronic, symptomatic, life-threatening illness; however, it is complex, with variable expression regarding impact on quality of life (QOL). This study investigated attitudes and comfort of physicians regarding palliative care (PC) for patients with PAH and explored potential barriers to PC in PAH. An internet-based, mixed-methods survey was distributed to Pulmonary Hypertension Clinicians and Researchers, a professional organization within the Pulmonary Hypertension Association. Only responses from physicians involved in clinical care of patients with PAH were analyzed. Of 355 clinicians/researchers, 79 (22%) returned surveys, including 76 (21%) providers involved in clinical care. Responding physicians were mainly pulmonologists (67%), practiced in university/academic medical centers (89%), had been in practice a mean of 12 ± 7 years, cared for a median of 100 PAH patients per year, and reported a high level of confidence in managing PAH (87%), advanced PAH-specific pharmacologic interventions (95%), and end-of-life care (88%). Smaller proportions were comfortable managing pain (62%) and QOL issues (78%). Most physicians (91%) reported utilizing PC consultation at least once in the prior year, primarily in the setting of end-of-life/active dying (59%), hospice referral (46%), or symptomatic dyspnea/impaired QOL (40%). The most frequent reasons for not referring patients to PC included nonapproval by the patient/family (51%) and concern that PC is "giving up hope" (43%). PAH may result in symptoms that impair QOL despite optimal PAH therapy; however, PC awareness and utilization for PAH providers is low. Opportunities may exist to integrate PC into care for PAH patients.
Keywords: palliative care; pulmonary arterial hypertension; quality of life; symptom control.
Figures
Similar articles
-
Symptom burden, quality of life, and attitudes toward palliative care in patients with pulmonary arterial hypertension: results from a cross-sectional patient survey.J Heart Lung Transplant. 2012 Oct;31(10):1102-8. doi: 10.1016/j.healun.2012.08.010. J Heart Lung Transplant. 2012. PMID: 22975100
-
A World of Maximalist Medicine: Physician Perspectives on Palliative Care and End-of-life for Patients With Pulmonary Arterial Hypertension.J Pain Symptom Manage. 2023 Apr;65(4):e329-e335. doi: 10.1016/j.jpainsymman.2022.11.027. Epub 2022 Dec 13. J Pain Symptom Manage. 2023. PMID: 36521765 Free PMC article.
-
Attitudes of Liver and Palliative Care Clinicians toward Specialist Palliative Care Consultation for Patients with End-Stage Liver Disease.J Palliat Med. 2019 Jul;22(7):804-813. doi: 10.1089/jpm.2018.0553. Epub 2019 Mar 20. J Palliat Med. 2019. PMID: 30892126
-
Pulmonary Arterial Hypertension: A Palliative Medicine Review of the Disease, Its Therapies, and Drug Interactions.J Pain Symptom Manage. 2020 Apr;59(4):932-943. doi: 10.1016/j.jpainsymman.2019.11.023. Epub 2019 Dec 2. J Pain Symptom Manage. 2020. PMID: 31805363 Review.
-
End-of-Life and Palliative Care Issues for Patients Living with Pulmonary Arterial Hypertension: Barriers and Opportunities.Semin Respir Crit Care Med. 2023 Dec;44(6):866-876. doi: 10.1055/s-0043-1770124. Epub 2023 Jul 17. Semin Respir Crit Care Med. 2023. PMID: 37459883 Review.
Cited by
-
The impact and financial burden of pulmonary arterial hypertension on patients and caregivers: results from a national survey.Medicine (Baltimore). 2017 Sep;96(39):e6783. doi: 10.1097/MD.0000000000006783. Medicine (Baltimore). 2017. PMID: 28953608 Free PMC article.
-
Roles of specific drug therapies for severe pulmonary arterial hypertension in palliative care: a case report.AME Case Rep. 2021 Jan 25;5:7. doi: 10.21037/acr-20-108. eCollection 2021. AME Case Rep. 2021. PMID: 33634247 Free PMC article.
-
Inpatient Palliative Care Use in Patients With Pulmonary Arterial Hypertension: Temporal Trends, Predictors, and Outcomes.Chest. 2020 Dec;158(6):2568-2578. doi: 10.1016/j.chest.2020.07.079. Epub 2020 Aug 12. Chest. 2020. PMID: 32800817 Free PMC article.
-
Pulmonary arterial hypertension: the burden of disease and impact on quality of life.Eur Respir Rev. 2015 Dec;24(138):621-9. doi: 10.1183/16000617.0063-2015. Eur Respir Rev. 2015. PMID: 26621976 Free PMC article. Review.
-
The PAH patient's perspective.Int J Cardiol Congenit Heart Dis. 2025 May 26;21:100596. doi: 10.1016/j.ijcchd.2025.100596. eCollection 2025 Sep. Int J Cardiol Congenit Heart Dis. 2025. PMID: 40546754 Free PMC article. Review.
References
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, et al. Survival in patients with primary pulmonary hypertension: results from a national prospective registry. Ann Intern Med 1991;115(5):343–349. - PubMed
-
- Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, Groves BM, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med 1996;334(5):296–301. - PubMed
-
- Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Hervé P, Rainisio M, Simonneau G. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol 2002;40(4):780–788. - PubMed
-
- McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation 2002;106(12):1477–1482. - PubMed
-
- Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med 2004;351(14):1425–1436. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
