

MELD scores and Child-Pugh classifications predict the outcomes of ERCP in cirrhotic patients with choledocholithiasis: a retrospective cohort study
- PMID: 25621696
- PMCID: PMC4602645
- DOI: 10.1097/MD.0000000000000433
MELD scores and Child-Pugh classifications predict the outcomes of ERCP in cirrhotic patients with choledocholithiasis: a retrospective cohort study
Abstract
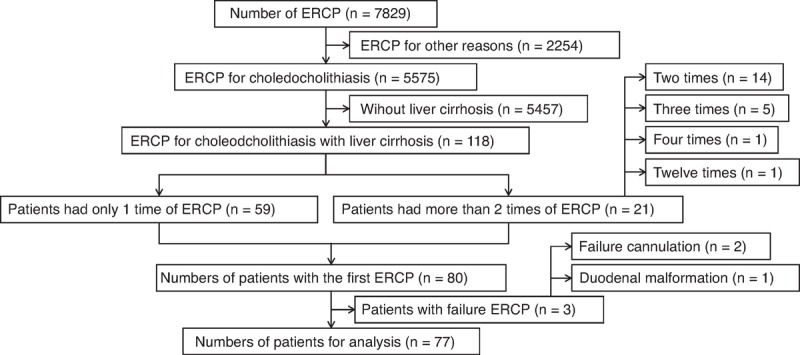
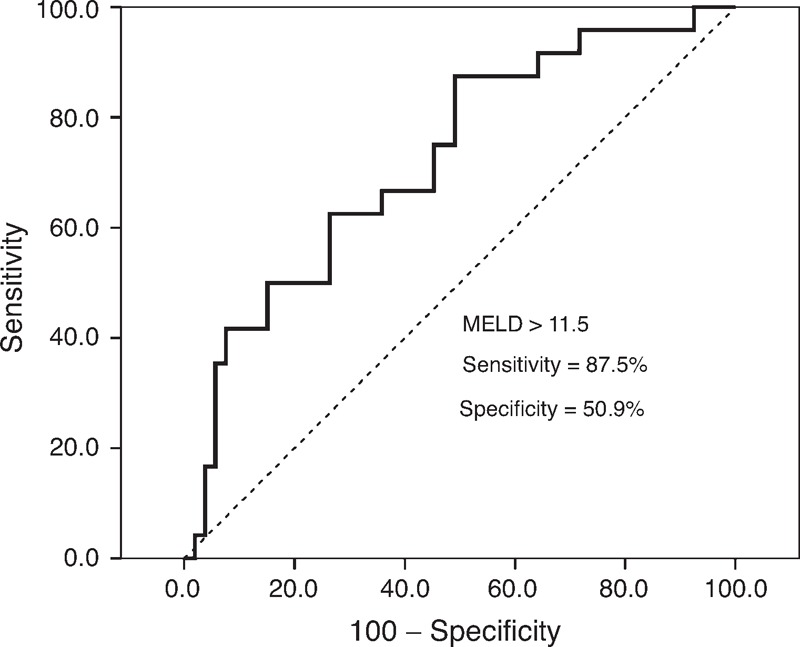
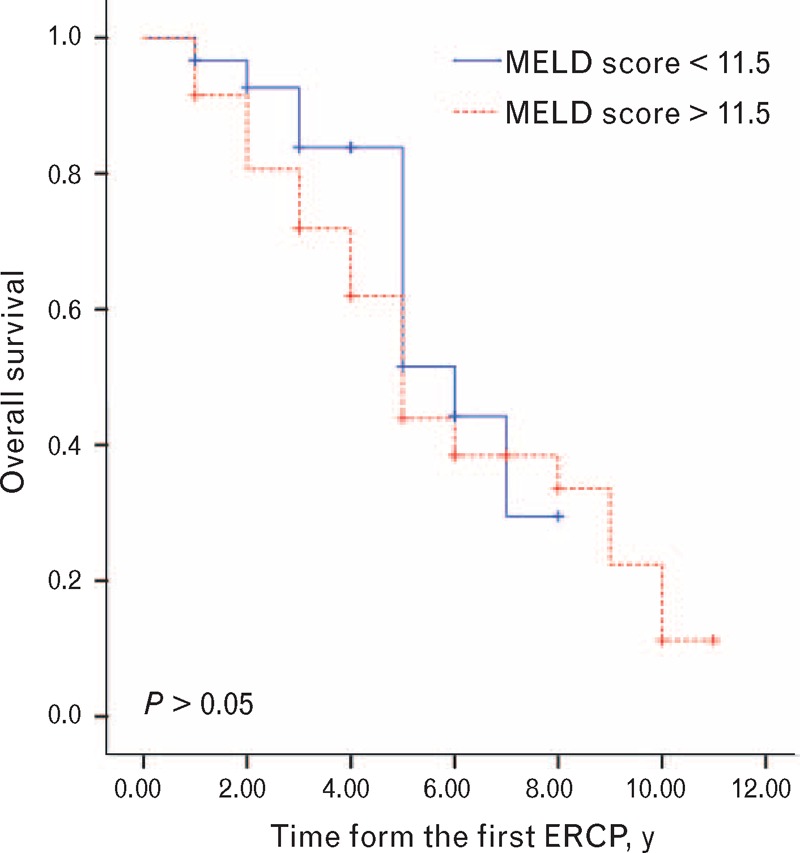
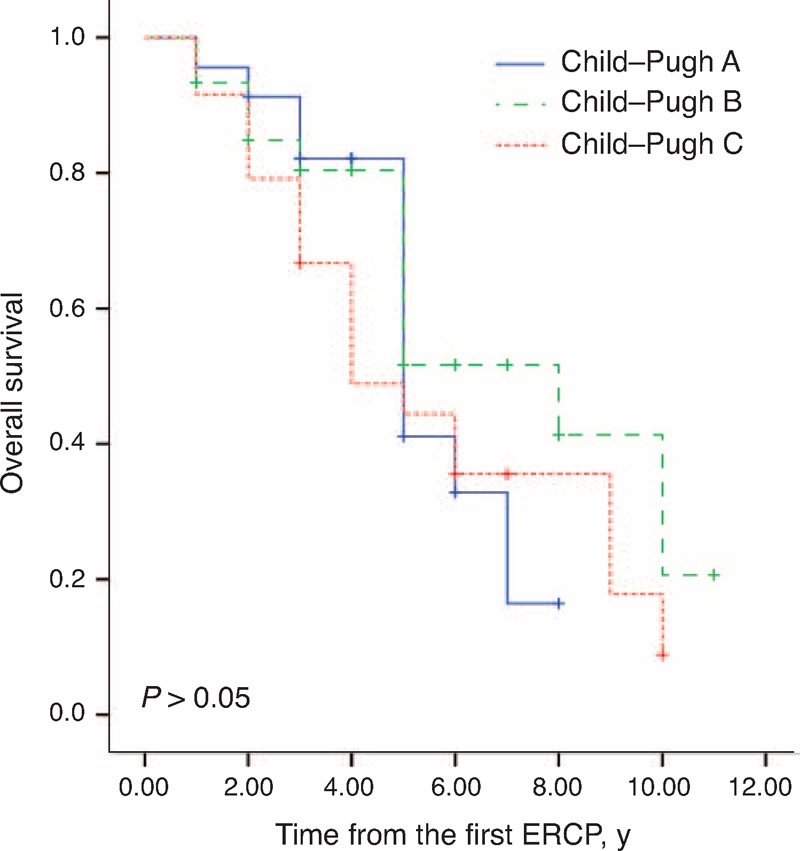
Endoscopic retrograde cholangiopancreatography (ERCP) is challenging in cirrhotic patients with choledocholithiasis. We evaluated the safety and efficacy of ERCP in cirrhotic patients with choledocholithiasis and accessed the model for end-stage liver disease (MELD) scores and Child-Pugh classifications for prediction of morbidity and mortality.From January 2000 to June 2014, 77 ERCP operations were performed in cirrhotic patients with choledocholithiasis. The data on operative complications were analyzed. MELD scores and Child-Pugh classifications were calculated and associated with operative outcomes and survival. Telephone follow-up was performed to determine survival situations.No death, perforation, or hemorrhage caused by gastroesophageal varices occurred as a result of the procedure. The rate of intraoperative hemorrhage was 13.0%, and the rate of postoperative morbidity was 27.3% including hemorrhage (18.2%), post-ERCP pancreatitis (6.1%), aggravated infection of the biliary tract (1.3%), hepatic encephalopathy (1.3%), and respiratory failure (1.3%). Four (5.2%) patients had both intraoperative and postoperative hemorrhage. Receiver operating characteristic analysis identified MELD scores higher than 11.5 as the best cutoff value for predicting complication incidence (95% confidence interval = 0.63-0.87). Twenty-one (44.7%) patients with a MELD score above 11.5 developed a complication, and 3 (10%) patients who had a lower MELD score developed a complication (P = 0.001). Both MELD score and Child-Pugh classification had prognostic value in patients without jaundice, although sex may result in different prognostic values based on the 2 scores. The rate of complications was not significantly different among patients with different Child-Pugh classifications. No significant difference was observed in patients with different MELD scores or Child-Pugh classifications in terms of median survival times.ERCP is an effective and safe procedure in cirrhotic patients with choledocholithiasis. MELD scores can predict the risk of operative complications, but Child-Pugh classification system scores do not predict the risk of complications.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Iber FL, Caruso G, Polepalle C, et al. Increasing prevalence of gallstones in male veterans with alcoholic cirrhosis. Am J Gastroenterol 1990; 85:1593–1596. - PubMed
-
- Acalovschi M, Badea R, Pascu M. Incidence of gallstones in liver cirrhosis. Am J Gastroenterol 1991; 86:1179–1181. - PubMed
-
- Chijiiwa K, Kozaki N, Naito T, et al. Treatment of choice for choledocholithiasis in patients with acute obstructive suppurative cholangitis and liver cirrhosis. Am J Surg 1995; 170:356–360. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
