

Clinical outcomes and cost effectiveness of accelerated diagnostic protocol in a chest pain center compared with routine care of patients with chest pain
- PMID: 25622029
- PMCID: PMC4306554
- DOI: 10.1371/journal.pone.0117287
Clinical outcomes and cost effectiveness of accelerated diagnostic protocol in a chest pain center compared with routine care of patients with chest pain
Abstract
Aims: The aim of this study was to compare in patients presenting with acute chest pain the clinical outcomes and cost-effectiveness of an accelerated diagnostic protocol utilizing contemporary technology in a chest pain unit versus routine care in an internal medicine department.
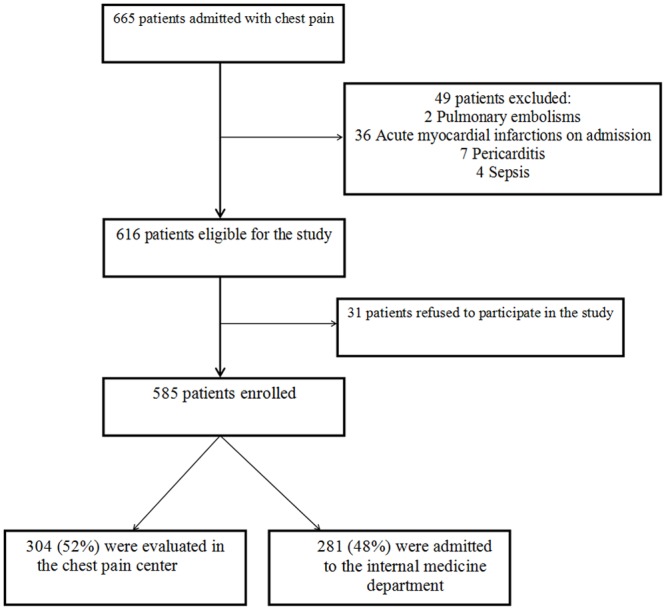
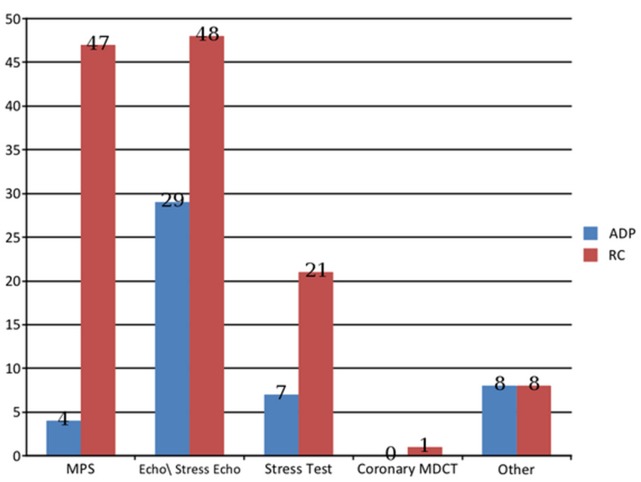
Methods and results: Hospital and 90-day course were prospectively studied in 585 consecutive low-moderate risk acute chest pain patients, of whom 304 were investigated in a designated chest pain center using a pre-specified accelerated diagnostic protocol, while 281 underwent routine care in an internal medicine ward. Hospitalization was longer in the routine care compared with the accelerated diagnostic protocol group (p<0.001). During hospitalization, 298 accelerated diagnostic protocol patients (98%) vs. 57 (20%) routine care patients underwent non-invasive testing, (p<0.001). Throughout the 90-day follow-up, diagnostic imaging testing was performed in 125 (44%) and 26 (9%) patients in the routine care and accelerated diagnostic protocol patients, respectively (p<0.001). Ultimately, most patients in both groups had non-invasive imaging testing. Accelerated diagnostic protocol patients compared with those receiving routine care was associated with a lower incidence of readmissions for chest pain [8 (3%) vs. 24 (9%), p<0.01], and acute coronary syndromes [1 (0.3%) vs. 9 (3.2%), p<0.01], during the follow-up period. The accelerated diagnostic protocol remained a predictor of lower acute coronary syndromes and readmissions after propensity score analysis [OR = 0.28 (CI 95% 0.14-0.59)]. Cost per patient was similar in both groups [($2510 vs. $2703 for the accelerated diagnostic protocol and routine care group, respectively, (p = 0.9)].
Conclusion: An accelerated diagnostic protocol is clinically superior and as cost effective as routine in acute chest pain patients, and may save time and resources.
Conflict of interest statement
Figures
Similar articles
-
Costs of an emergency department-based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial.JAMA. 1997 Nov 26;278(20):1670-6. JAMA. 1997. PMID: 9388086 Clinical Trial.
-
Long-term experience with an accelerated protocol for diagnosis of chest pain.Arch Pathol Lab Med. 2000 Oct;124(10):1434-9. doi: 10.5858/2000-124-1434-LTEWAA. Arch Pathol Lab Med. 2000. PMID: 11035571
-
A 2-hour diagnostic protocol for possible cardiac chest pain in the emergency department: a randomized clinical trial.JAMA Intern Med. 2014 Jan;174(1):51-8. doi: 10.1001/jamainternmed.2013.11362. JAMA Intern Med. 2014. PMID: 24100783 Clinical Trial.
-
Evaluation of chest pain suspicious for acute coronary syndrome: use of an accelerated diagnostic protocol in a chest pain evaluation unit.Am J Cardiol. 2000 Mar 9;85(5A):40B-48B; discussion 49B. doi: 10.1016/s0002-9149(00)00755-4. Am J Cardiol. 2000. PMID: 11076130 Review.
-
Acute ischemic syndromes. Chest pain center concept.Cardiol Clin. 2002 Feb;20(1):117-36. doi: 10.1016/s0733-8651(03)00069-9. Cardiol Clin. 2002. PMID: 11845539 Review.
Cited by
-
Feasibility and Safety of Evaluating Patients with Prior Coronary Artery Disease Using an Accelerated Diagnostic Algorithm in a Chest Pain Unit.PLoS One. 2016 Sep 26;11(9):e0163501. doi: 10.1371/journal.pone.0163501. eCollection 2016. PLoS One. 2016. PMID: 27669521 Free PMC article.
-
Health Care Quality Improvement for ST-Segment Elevation Myocardial Infarction: A Retrospective Study Based on Propensity-Score Matching Analysis.Int J Environ Res Public Health. 2021 Jun 4;18(11):6045. doi: 10.3390/ijerph18116045. Int J Environ Res Public Health. 2021. PMID: 34199816 Free PMC article.
-
Change to costs and lengths of stay in the emergency department and the Brisbane protocol: an observational study.BMJ Open. 2016 Feb 25;6(2):e009746. doi: 10.1136/bmjopen-2015-009746. BMJ Open. 2016. PMID: 26916691 Free PMC article.
References
-
- Zalenski RJ, Rydman RJ, McCarren M, Roberts RR, Jovanovic B, et al. (1997) Feasibility of a rapid diagnostic protocol for an emergency department chest pain unit. Ann Emerg Med 29(1):99–108. - PubMed
-
- Graff LG, Dallara J, Ross MA, Joseph AJ, Itzcovitz J, et al. (1997) Impact on the care of the emergency department chest pain patient from the chest pain evaluation registry (CHEPER) study. Am J Cardiol 80(5):563–568. - PubMed
-
- Gibler WB (1994) Chest pain evaluation in the ED: beyond triage [Editorial]. Am J Emerg Med 12(1):121–122. - PubMed
-
- Rubinshtein R, Halon DA, Kogan A, Jaffe R, Karkabi B, et al. (2006) Initial experience with a cardiologist-based chest pain unit in an emergency department in Israel. Isr Med Assoc J 8(5):329–332. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
