

Optimizing the detection of recent tuberculosis infection in children in a high tuberculosis-HIV burden setting
- PMID: 25622087
- PMCID: PMC4407483
- DOI: 10.1164/rccm.201406-1165OC
Optimizing the detection of recent tuberculosis infection in children in a high tuberculosis-HIV burden setting
Abstract
Rationale: Children who are young, malnourished, and infected with HIV have significant risk of tuberculosis (TB) morbidity and mortality following TB infection. Treatment of TB infection is hindered by poor detection and limited pediatric data.
Objectives: Identify improved testing to detect pediatric TB infection.
Methods: This was a prospective community-based study assessing use of the tuberculin skin test and IFN-γ release assays among children (n = 1,343; 6 mo to <15 yr) in TB-HIV high-burden settings; associations with child characteristics were measured.
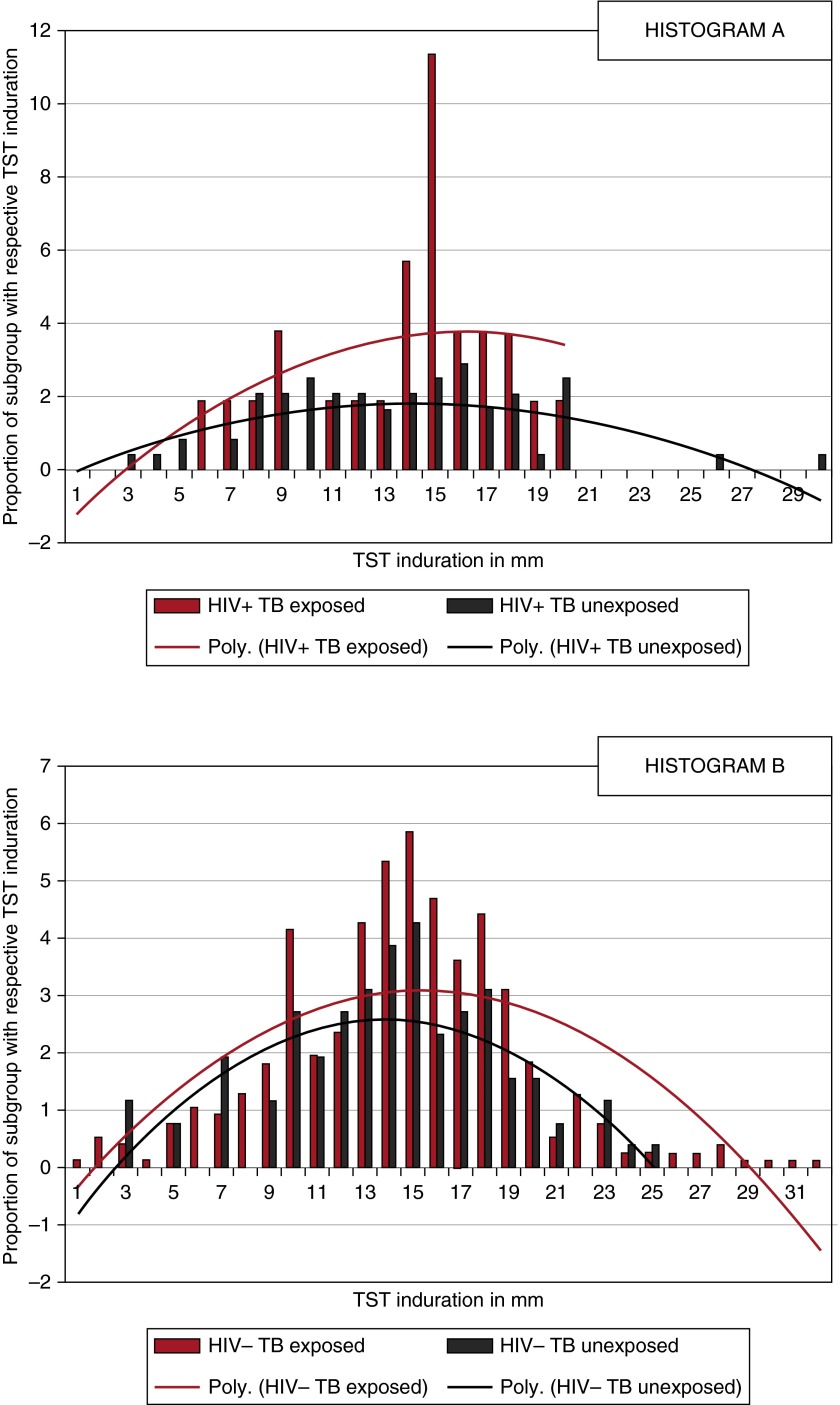
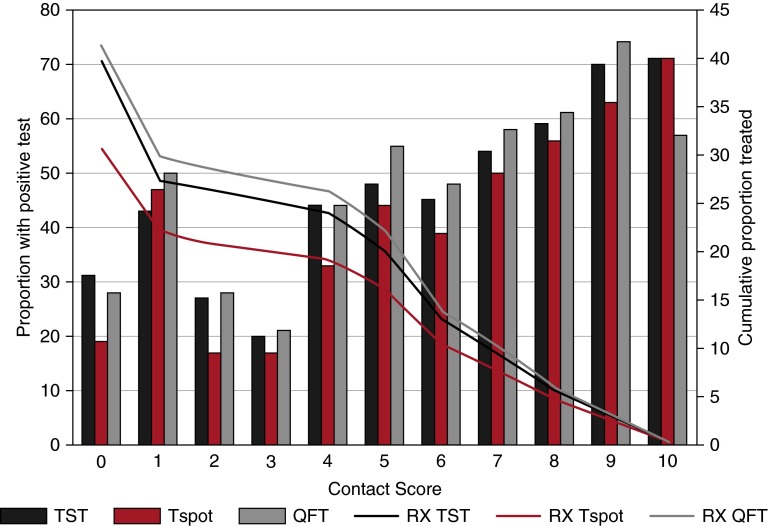
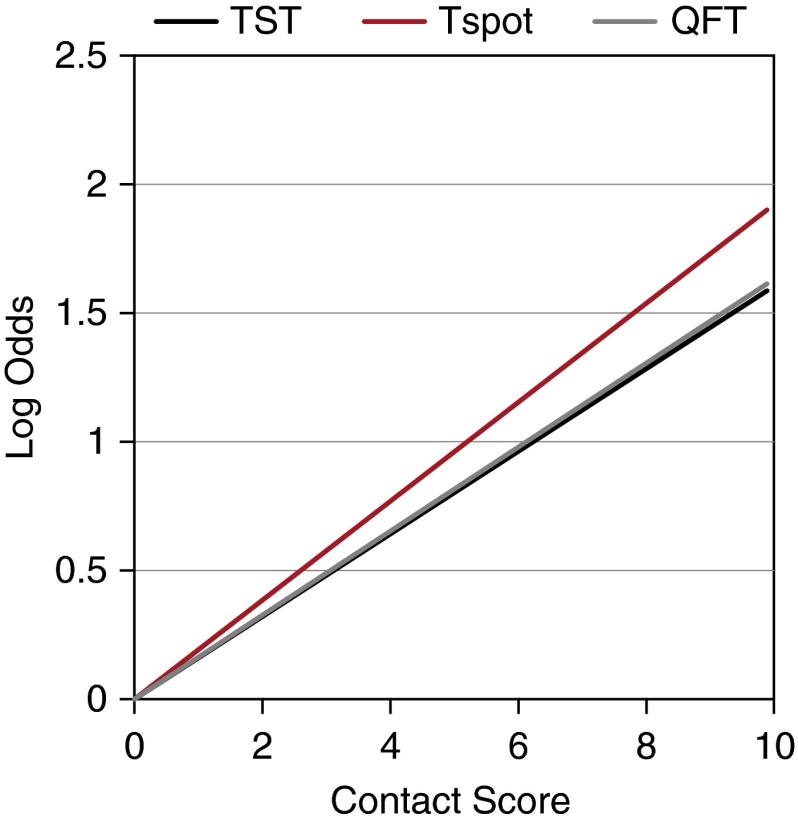
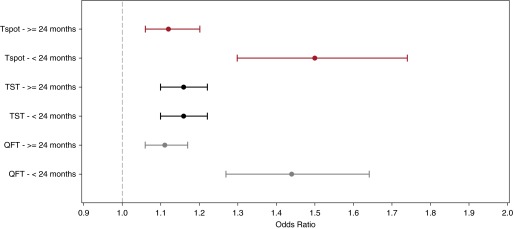
Measurements and main results: Contact tracing detects TB in 8% of child contacts within 3 months of exposure. Among children with no documented contact, tuberculin skin test and QuantiFERON-TB Gold In-Tube positivity was greater than T-SPOT.TB. Nearly 8% of children had IFN-γ release assay positive and skin test negative discordance. In a model accounting for confounders, all tests correlate with TB contact, but IFN-γ release assays correlate better than the tuberculin skin test (P = 0.0011). Indeterminate IFN-γ release assay results were not associated with age. Indeterminate QuantiFERON-TB Gold In-Tube results were more frequent in children infected with HIV (4.7%) than uninfected with HIV (1.9%), whereas T-SPOT.TB indeterminates were rare (0.2%) and not affected by HIV status. Conversion and reversion were not associated with HIV status. Among children infected with HIV, tests correlated less with contact as malnutrition worsened.
Conclusions: Where resources allow, use of IFN-γ release assays should be considered in children who are young, recently exposed, and infected with HIV because they may offer advantages compared with the tuberculin skin test for identifying TB infection, and improve targeted, cost-effective delivery of preventive therapy. Affordable tests of infection could dramatically impact global TB control.
Keywords: HIV; IFN-γ release tests; latent tuberculosis infection; pediatrics; tuberculin test.
Figures
Similar articles
-
Latent Tuberculosis Infection Screening and 2-Year Outcome in Antiretroviral-Naive HIV-Infected Patients in a Low-Prevalence Country.Ann Am Thorac Soc. 2015 Aug;12(8):1138-45. doi: 10.1513/AnnalsATS.201412-600OC. Ann Am Thorac Soc. 2015. PMID: 26213798
-
Identifying predictors of interferon-γ release assay results in pediatric latent tuberculosis: a protective role of bacillus Calmette-Guerin?: a pTB-NET collaborative study.Am J Respir Crit Care Med. 2012 Aug 15;186(4):378-84. doi: 10.1164/rccm.201201-0026OC. Epub 2012 Jun 14. Am J Respir Crit Care Med. 2012. PMID: 22700862 Free PMC article.
-
Performance of commercial blood tests for the diagnosis of latent tuberculosis infection in children and adolescents.Pediatrics. 2009 Mar;123(3):e419-24. doi: 10.1542/peds.2008-1722. Pediatrics. 2009. PMID: 19254978
-
Interferon-γ release assays or tuberculin skin test for detection and management of latent tuberculosis infection: a systematic review and meta-analysis.Lancet Infect Dis. 2020 Dec;20(12):1457-1469. doi: 10.1016/S1473-3099(20)30276-0. Epub 2020 Jul 13. Lancet Infect Dis. 2020. PMID: 32673595
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
Cited by
-
T-SPOT.TB Performance in Routine Pediatric Practice in a Low TB Burden Setting.Pediatr Infect Dis J. 2018 Apr;37(4):292-297. doi: 10.1097/INF.0000000000001792. Pediatr Infect Dis J. 2018. PMID: 29140933 Free PMC article.
-
THE ROLE OF INTERFERON-GAMMA RELEASE ASSAYS IN DIAGNOSIS OF LATENT TUBERCULOSIS INFECTION IN CHILDREN.Acta Clin Croat. 2023 Nov;62(3):527-538. doi: 10.20471/acc.2023.62.03.15. Acta Clin Croat. 2023. PMID: 39310695 Free PMC article. Review.
-
Hepatic and Intra-abdominal Tuberculosis: 2016 Update.Curr Infect Dis Rep. 2016 Dec;18(12):45. doi: 10.1007/s11908-016-0546-5. Curr Infect Dis Rep. 2016. PMID: 27796776 Review.
-
Update in Mycobacterium tuberculosis lung disease 2014.Am J Respir Crit Care Med. 2015 Oct 1;192(7):793-8. doi: 10.1164/rccm.201505-1009UP. Am J Respir Crit Care Med. 2015. PMID: 26426784 Free PMC article. Review. No abstract available.
-
Comparison of Interferon-γ Release Assays and the Tuberculin Skin Test for Diagnosis of Tuberculosis in Human Immunodeficiency Virus: A Systematic Review.Tuberc Respir Dis (Seoul). 2018 Jan;81(1):59-72. doi: 10.4046/trd.2017.0072. Epub 2017 Dec 13. Tuberc Respir Dis (Seoul). 2018. PMID: 29256218 Free PMC article.
References
-
- Sloot R, Schim van der Loeff MF, Kouw PM, Borgdorff MW. Risk of tuberculosis after recent exposure. A 10-year follow-up study of contacts in Amsterdam. Am J Respir Crit Care Med. 2014;190:1044–1052. - PubMed
-
- Marais BJ, Gie RP, Schaaf HS, Hesseling AC, Obihara CC, Starke JJ, Enarson DA, Donald PR, Beyers N. The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tubercul Lung Dis. 2004;8:392–402. - PubMed
-
- Woldehanna S Volmink J. Treatment of latent tuberculosis infection in HIV infected persons. Cochrane Databases Syst Rev. 2004;(1):CD000171. - PubMed
-
- Hsu KH. Isoniazid in the prevention and treatment of tuberculosis. A 20-year study of the effectiveness in children. JAMA. 1974;229:528–533. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
