

Antihormonal agents as a strategy to improve the effect of chemo-radiation in cervical cancer: in vitro and in vivo study
- PMID: 25622528
- PMCID: PMC4311459
- DOI: 10.1186/s12885-015-1016-4
Antihormonal agents as a strategy to improve the effect of chemo-radiation in cervical cancer: in vitro and in vivo study
Abstract
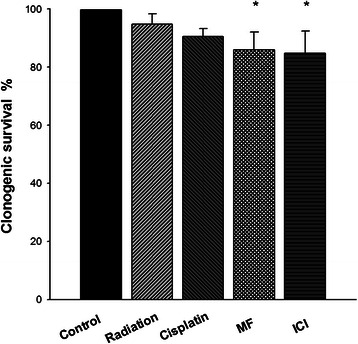
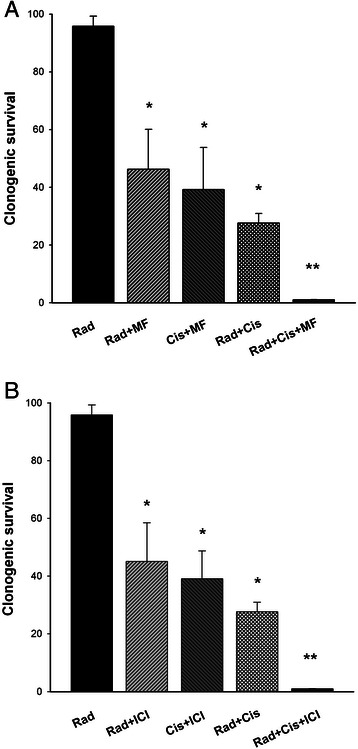
Background: Over the past few years, the concurrent use of cisplatin-based chemotherapy and radiation therapy has dramatically improved the local response and increased overall survival in early-stage cervical cancer. However, for the advanced stages of the disease this standard treatment has proved insufficient. We investigated the capacity of Mifepristone and ICI 182,780, which are anti-progestin and anti-estrogen drugs, respectively, to act as chemo-radiosensitizing agents in cervical cancer cells and cervix xenografts.
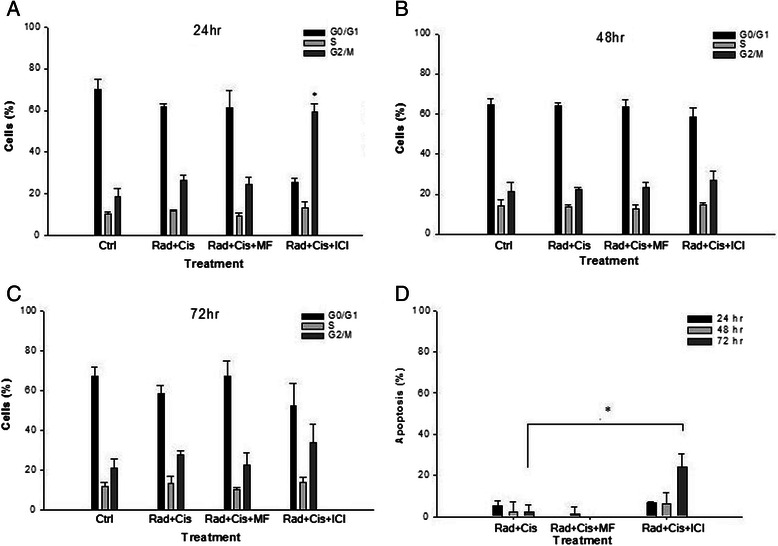
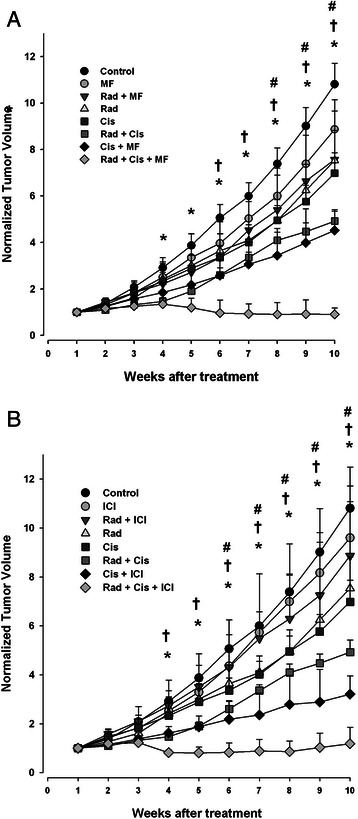
Methods: The effect of chemo-radiation alone or combined with Mifepristone or ICI 182,780 was evaluated in HeLa cells and with tumor growth in cervix xenografts. After concomitant chemo-radiotherapy, the effect of each of these antihormonal agents on apoptosis (determined by Annexing V assay) and the cell cycle phases were determined by flow cytometry. The expression of angiogenic factor VEGF in tumor samples was determined using quantitative RT-PCR analysis of VEGF gene expression.
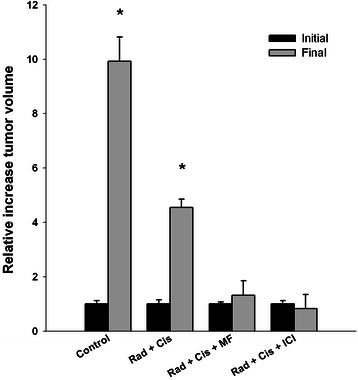
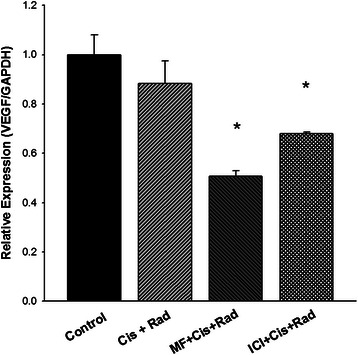
Results: Compared to radiation alone or radiation/cisplatin therapy, there was significantly higher cytotoxicity and a greater antitumoral effect with the combined application of radiation/cisplatin and Mifepristone or ICI 182,780. Analyses of the apoptosis and cell cycle demonstrated changes only with ICI, not with Mifepristone, when was applied in combination with radiation/cisplatin. The analysis of VEGF mRNA expression levels in tumors at the end of the study demonstrated a significant inhibition, compared to radiation only or the radiation/cisplatin treatment, after concurrent chemo-radiotherapy and each one of the antihormonal drugs.
Conclusion: Mifepristone and ICI 182,780 may be potentially promising chemo-radiosensitizing compounds to be used in combination with ionizing irradiation and cisplatin in the treatment of patients with advanced cervical cancer.
Figures
Similar articles
-
Synergistic effects of ICI 182,780 on the cytotoxicity of cisplatin in cervical carcinoma cell lines.Cancer Chemother Pharmacol. 2004 Jun;53(6):533-40. doi: 10.1007/s00280-003-0760-3. Epub 2004 Jan 29. Cancer Chemother Pharmacol. 2004. PMID: 15138713
-
The cisplatin-irradiation combination suggests that apoptosis is not a major determinant of clonogenic death.Anticancer Drugs. 2007 Jul;18(6):659-67. doi: 10.1097/CAD.0b013e328087388f. Anticancer Drugs. 2007. PMID: 17762394
-
Cisplatin cytotoxicity is increased by mifepristone in cervical carcinoma: an in vitro and in vivo study.Oncol Rep. 2009 Nov;22(5):1237-45. doi: 10.3892/or_00000560. Oncol Rep. 2009. PMID: 19787245
-
Combined radiation therapy and chemotherapy for carcinoma of the cervix.Cancer J. 2001 Mar-Apr;7(2):86-94. Cancer J. 2001. PMID: 11324770 Review.
-
Targeting the CXCL12/CXCR4 pathway and myeloid cells to improve radiation treatment of locally advanced cervical cancer.Int J Cancer. 2018 Sep 1;143(5):1017-1028. doi: 10.1002/ijc.31297. Epub 2018 Mar 5. Int J Cancer. 2018. PMID: 29417588 Review.
Cited by
-
Vorinostat enhances the cisplatin-mediated anticancer effects in small cell lung cancer cells.BMC Cancer. 2016 Nov 7;16(1):857. doi: 10.1186/s12885-016-2888-7. BMC Cancer. 2016. PMID: 27821078 Free PMC article.
-
Pharmacokinetics and Anti-Tumor Efficacy of PEGylated Liposomes Co-Loaded with Cisplatin and Mifepristone.Pharmaceuticals (Basel). 2023 Sep 22;16(10):1337. doi: 10.3390/ph16101337. Pharmaceuticals (Basel). 2023. PMID: 37895808 Free PMC article.
-
CDS-1548 induces apoptosis in HeLa cells by activating caspase 3.Oncol Lett. 2019 Aug;18(2):1881-1887. doi: 10.3892/ol.2019.10511. Epub 2019 Jun 21. Oncol Lett. 2019. PMID: 31423257 Free PMC article.
-
Computational repositioning and preclinical validation of mifepristone for human vestibular schwannoma.Sci Rep. 2018 Apr 3;8(1):5437. doi: 10.1038/s41598-018-23609-7. Sci Rep. 2018. PMID: 29615643 Free PMC article.
-
Molecular mechanisms of cisplatin resistance in cervical cancer.Drug Des Devel Ther. 2016 Jun 7;10:1885-95. doi: 10.2147/DDDT.S106412. eCollection 2016. Drug Des Devel Ther. 2016. PMID: 27354763 Free PMC article. Review.
References
-
- Bosch FX. Epidemiology of human papillomavirus infections: new options for cervical cancer prevention. Salud Publica Mex. 2003;45:S326–39. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
