

Cognitive-behavioral therapy for insomnia in knee osteoarthritis: a randomized, double-blind, active placebo-controlled clinical trial
- PMID: 25623343
- PMCID: PMC6040809
- DOI: 10.1002/art.39048
Cognitive-behavioral therapy for insomnia in knee osteoarthritis: a randomized, double-blind, active placebo-controlled clinical trial
Abstract
Objective: Insomnia is prevalent among patients with knee osteoarthritis (OA). Research indicates that sleep disruption may amplify clinical pain by altering central pain modulation, suggesting that treatment of insomnia may improve pain. The aims of this study were to evaluate the efficacy of cognitive-behavioral therapy for insomnia (CBT-I) in patients with knee OA, to determine whether improvements in sleep predict reduced pain, and to determine whether alterations in pain modulation mediate improvements in clinical pain.
Methods: We conducted a randomized, double-blind, active placebo-controlled clinical trial of CBT-I in 100 patients with knee OA and insomnia (mean ± SD age 59.4 ± 9.5 years). Patients were randomized (1:1) to receive either 8 sessions of CBT-I or behavioral desensitization (placebo). We conducted in-home polysomnography (PSG), diary assessment, and sensory tests of pain modulation at baseline, posttreatment, 3 months, and 6 months.
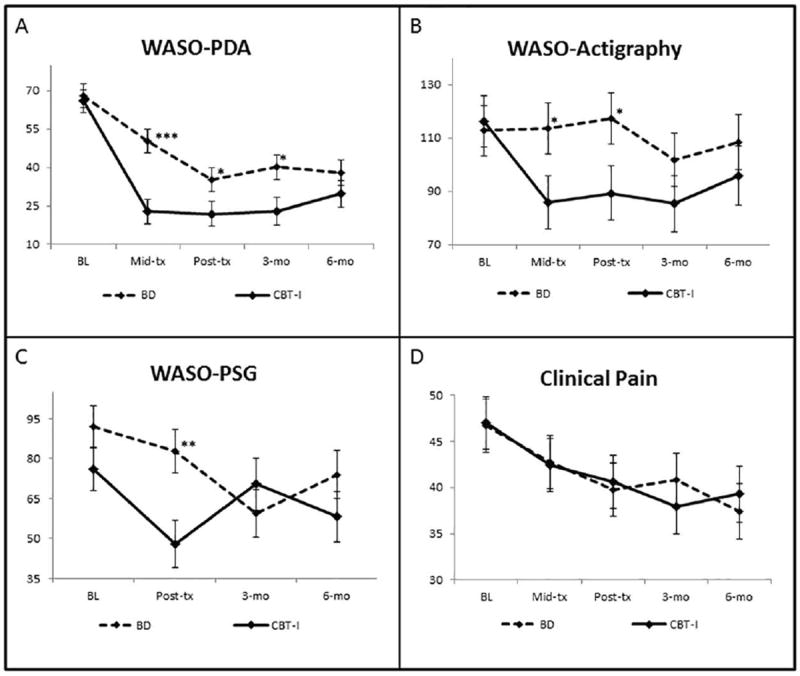
Results: Intent-to-treat analyses demonstrated substantial improvement in sleep in both groups of patients. Patients in the CBT-I group had significantly greater reductions in wake after sleep onset (WASO), as measured by patient diary and PSG. Patients in both groups reported significant and comparable reductions in pain over 6 months, with one-third reporting a 30% reduction in pain severity. Baseline-to-posttreatment reductions in WASO as measured by diary and PSG predicted subsequent decreases in clinical pain. This effect was significantly greater for CBT-I compared with behavioral desensitization. No significant changes in laboratory measures of pain modulation were observed.
Conclusion: Compared with active placebo, CBT-I was efficacious in reducing sleep maintenance insomnia. CBT-I decreased clinical pain, but not pain modulation, suggesting that it has the potential to augment pain management in knee OA. Future work is needed to identify the mechanisms by which improved sleep reduces clinical pain.
Trial registration: ClinicalTrials.gov NCT00592449.
© 2015, American College of Rheumatology.
Figures

References
-
- Felson DT. An update on the pathogenesis and epidemiology of osteoarthritis. Radiol Clin North Am. 2004;42(1):1–9. v. - PubMed
-
- Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis. Lancet. 2005;365(9463):965–73. - PubMed
-
- Lanes SF, Lanza LL, Radensky PW, Yood RA, Meenan RF, Walker AM, et al. Resource utilization and cost of care for rheumatoid arthritis and osteoarthritis in a managed care setting: the importance of drug and surgery costs. Arthritis Rheum. 1997;40(8):1475–81. - PubMed
-
- Creamer P, Lethbridge-Cejku M, Hochberg MC. Factors associated with functional impairment in symptomatic knee osteoarthritis. Rheumatology (Oxford) 2000;39(5):490–6. - PubMed
-
- Dominick KL, Ahern FM, Gold CH, Heller DA. Health-related quality of life and health service use among older adults with osteoarthritis. Arthritis Rheum. 2004;51(3):326–31. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
