

Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot
- PMID: 25623907
- PMCID: PMC4437857
- DOI: 10.1016/j.jtcvs.2014.11.085
Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot
Abstract
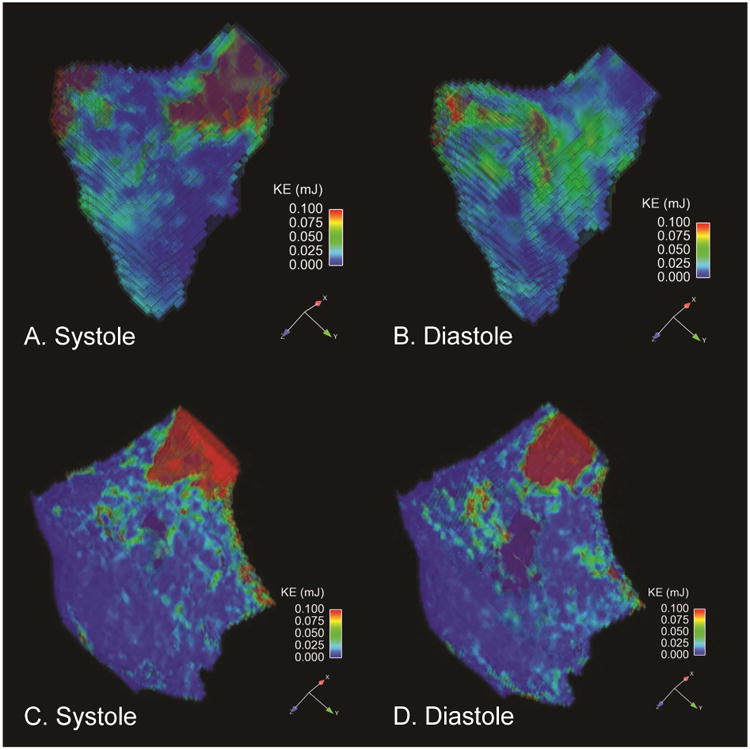
Objective: Ventricular kinetic energy measurements may provide a novel imaging biomarker of declining ventricular efficiency in patients with repaired tetralogy of Fallot. Our purpose was to assess differences in ventricular kinetic energy with 4-dimensional flow magnetic resonance imaging between patients with repaired tetralogy of Fallot and healthy volunteers.
Methods: Cardiac magnetic resonance, including 4-dimensional flow magnetic resonance imaging, was performed at rest in 10 subjects with repaired tetralogy of Fallot and 9 healthy volunteers using clinical 1.5T and 3T magnetic resonance imaging scanners. Right and left ventricular kinetic energy (KERV and KELV), main pulmonary artery flow (QMPA), and aortic flow (QAO) were quantified using 4-dimensional flow magnetic resonance imaging data. Right and left ventricular size and function were measured using standard cardiac magnetic resonance techniques. Differences in peak systolic KERV and KELV in addition to the QMPA/KERV and QAO/KELV ratios between groups were assessed. Kinetic energy indices were compared with conventional cardiac magnetic resonance parameters.
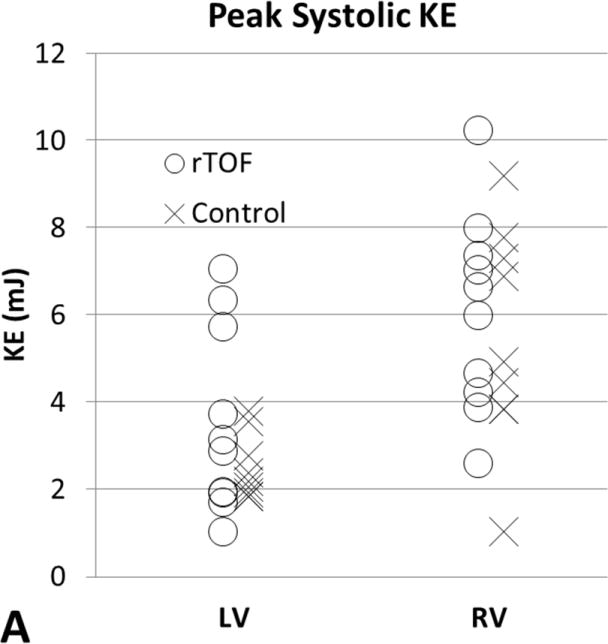
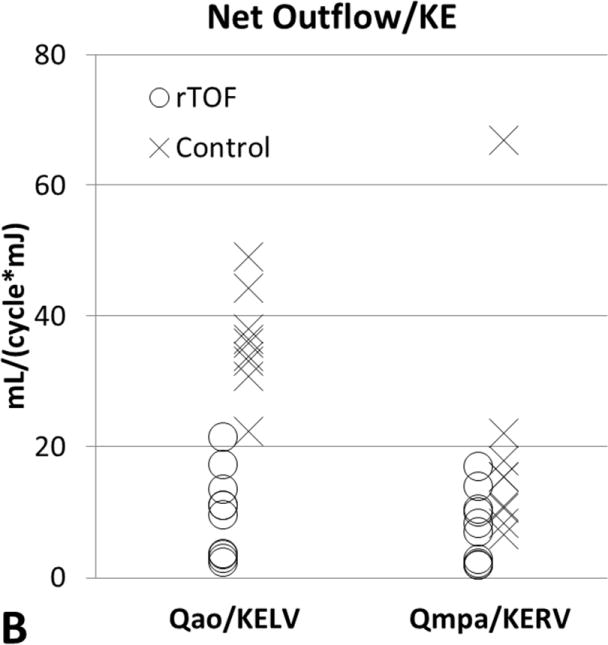
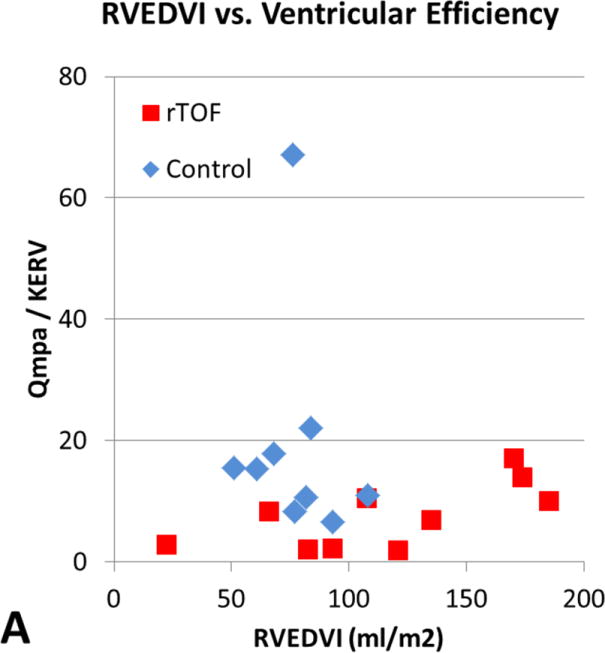
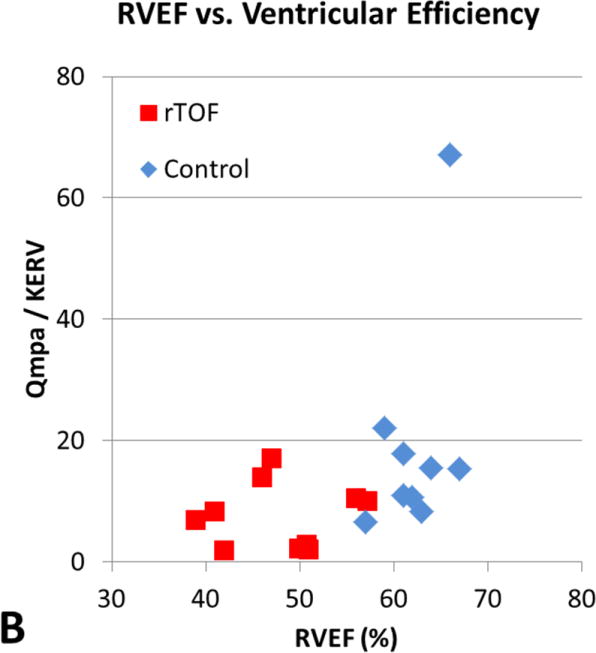
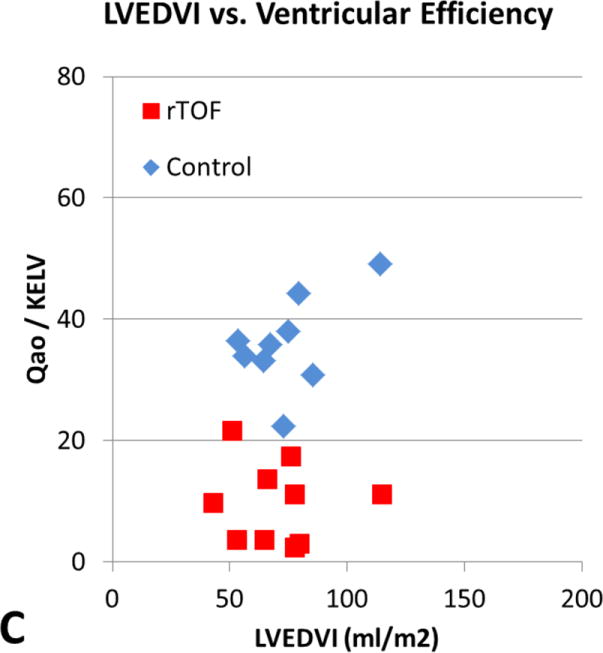
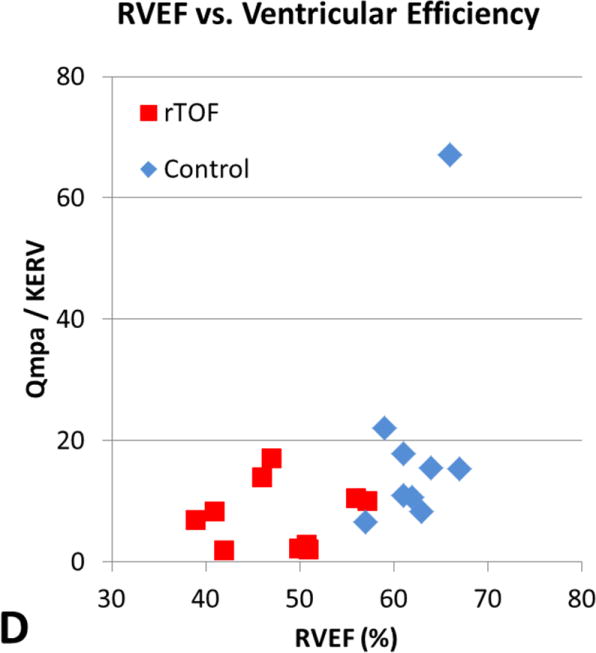
Results: Peak systolic KERV and KELV were higher in patients with repaired tetralogy of Fallot (6.06 ± 2.27 mJ and 3.55 ± 2.12 mJ, respectively) than in healthy volunteers (5.47 ± 2.52 mJ and 2.48 ± 0.75 mJ, respectively), but were not statistically significant (P = .65 and P = .47, respectively). The QMPA/KERV and QAO/KELV ratios were lower in patients with repaired tetralogy of Fallot (7.53 ± 5.37 mL/[cycle mJ] and 9.65 ± 6.61 mL/[cycle mJ], respectively) than in healthy volunteers (19.33 ± 18.52 mL/[cycle mJ] and 35.98 ± 7.66 mL/[cycle mJ], respectively; P < .05). QMPA/KERV and QAO/KELV were weakly correlated to ventricular size and function.
Conclusions: Greater ventricular kinetic energy is necessary to generate flow in the pulmonary and aortic circulations in repaired tetralogy of Fallot. Quantification of ventricular kinetic energy in patients with repaired tetralogy of Fallot is a new observation. Future studies are needed to determine whether changes in ventricular kinetic energy can provide earlier evidence of ventricular dysfunction and guide future medical and surgical interventions.
Copyright © 2015 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Ventricular function in tetralogy of Fallot: A waste of energy.J Thorac Cardiovasc Surg. 2015 May;149(5):1348. doi: 10.1016/j.jtcvs.2014.12.042. Epub 2014 Dec 24. J Thorac Cardiovasc Surg. 2015. PMID: 25648480 No abstract available.
References
-
- Starr JP. Tetralogy of Fallot: yesterday and today. World J Surg. 2010;34(4):658–668. - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Adamson L, Vohra HA, Haw MP. Does pulmonary valve replacement post repair of tetralogy of Fallot improve right ventricular function? Interact Cardiovasc Thorac Surg. 2009;9:520–527. - PubMed
-
- Khalaf A, Tani D, Tadros S, Madan S. Right- and left- ventricular strain evaluation in repaired pediatric Tetralogy of Fallot patients using magnetic resonance tagging. Pediatr Cardiol. 2013;34:1206–1211. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
