

Retroperitoneal lymph node dissection (RPLND) for malignant phenotype Leydig cell tumours of the testis: a 10-year experience
- PMID: 25625040
- PMCID: PMC4300307
- DOI: 10.1186/s40064-014-0781-x
Retroperitoneal lymph node dissection (RPLND) for malignant phenotype Leydig cell tumours of the testis: a 10-year experience
Abstract
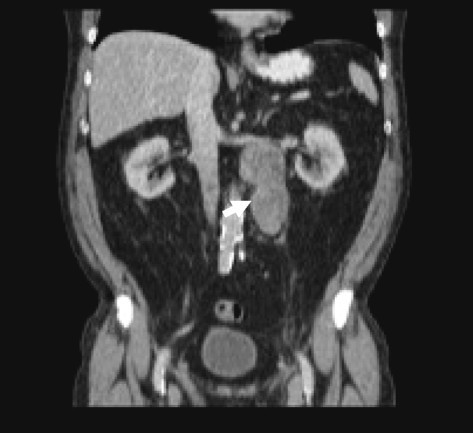
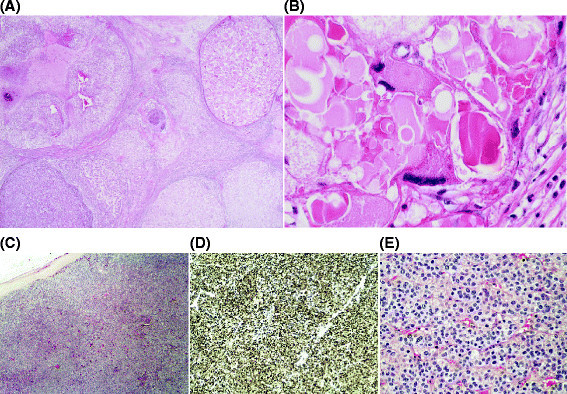
Retroperitoneal lymph node dissection (RPLND) is a prognostic, palliative, and potentially therapeutic procedure for patients with malignant phenotype Leydig cell tumours of the testis. We reviewed the records of patients diagnosed with malignant phenotype Leydig cell tumours of the testis treated by RPLND. Modified template dissection was performed in all cases with extra-template excision of tumour mass in Stage II disease. Routine clinico-radiological follow-up was performed. Six open RPLNDs (1 re-do procedure) were performed on 5 patients diagnosed with Stage I (n = 3) and Stage II (n = 2) malignant phenotype Leydig cell tumour of the testis. Median age = 63 years (range = 55-72). Median peri-operative blood loss = 1500 ml (range = 500-1500 ml). Median operating time = 6 h (range = 4.5-6.5). Two patients with Stage II disease developed post-operative complications of acute kidney injury (n = 1) and pneumonia (n = 1). Median length of stay was 8 days (range = 6-11). RPLND specimens from patients with Stage I were tumour-free, whilst patients with Stage II disease had evidence of metastatic tumour. At latest follow-up (median = 13 months, range = 7-22), no patient with Stage I disease had radiological evidence of recurrence, however the two patients with Stage II disease had died due to tumour recurrence at 13 months and 36 months. RPLND for malignant phenotype Leydig cell testicular tumours appears to be well tolerated. Despite surgery, overall outcomes for Stage II appear to be poor due to the disease phenotype. Larger prospective multi-centre studies are required to determine the definitive criteria for surgery in Stage I disease.
Keywords: Leydig cell tumour; Retroperitoneal lymph node dissection (RPLND); Testicular cancer.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
