

Hypoglossal nerve palsy after airway management for general anesthesia: an analysis of 69 patients
- PMID: 25625257
- PMCID: PMC4308816
- DOI: 10.1213/ANE.0000000000000495
Hypoglossal nerve palsy after airway management for general anesthesia: an analysis of 69 patients
Abstract
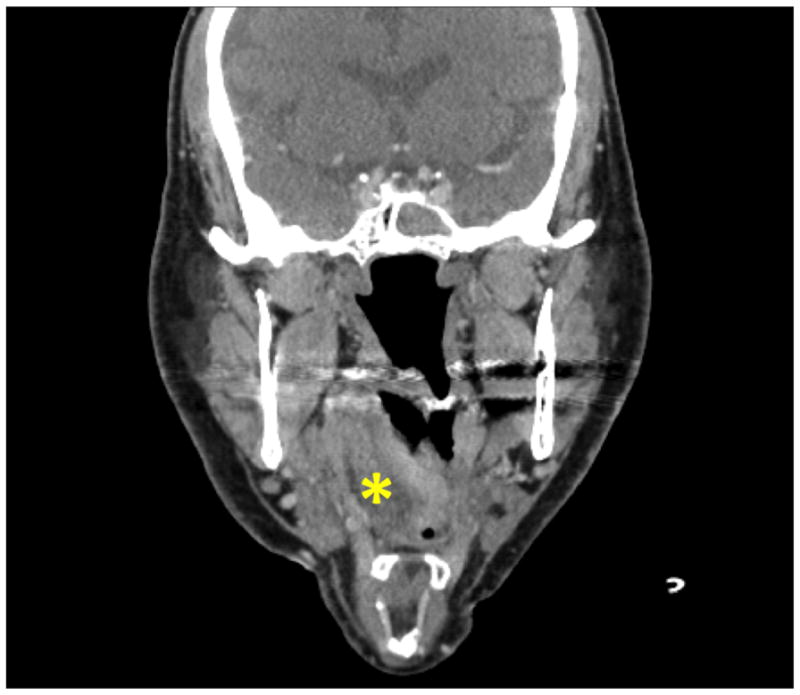
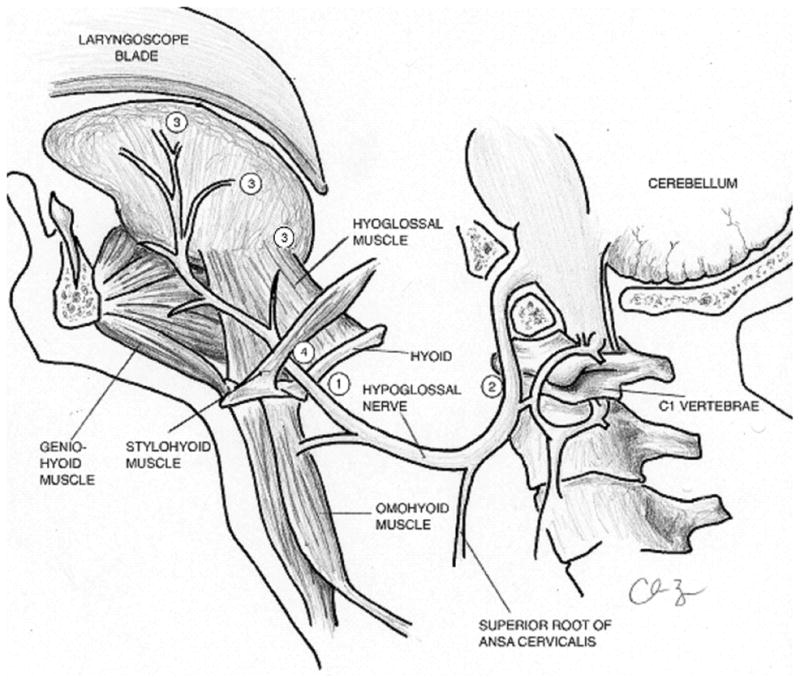
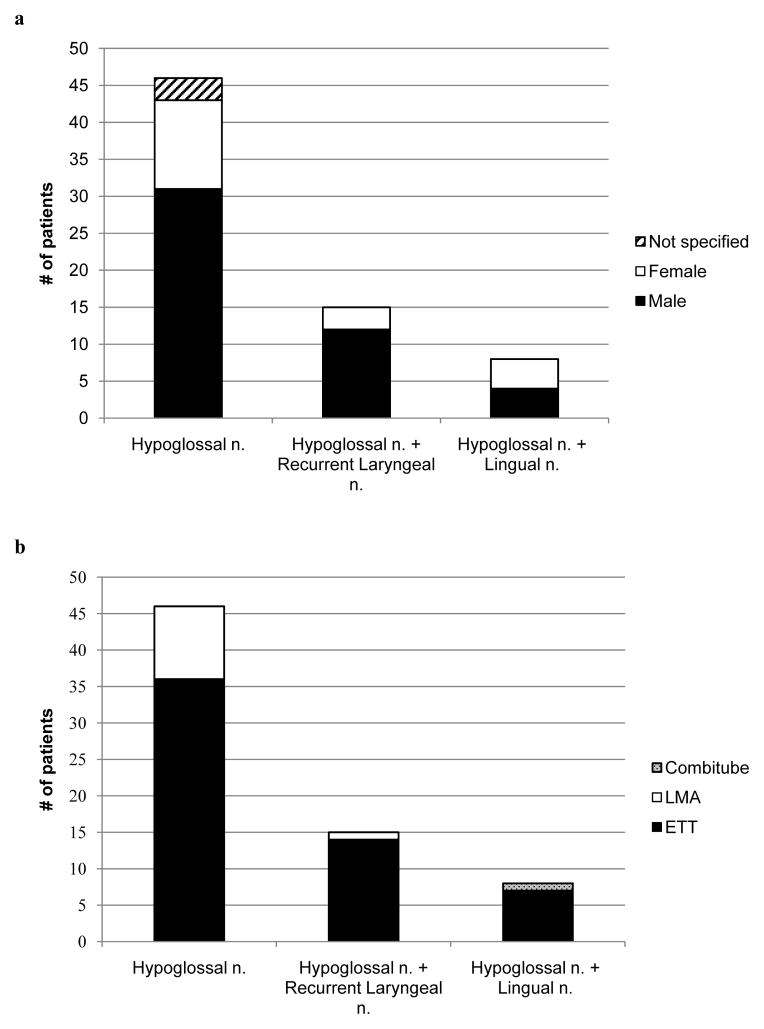
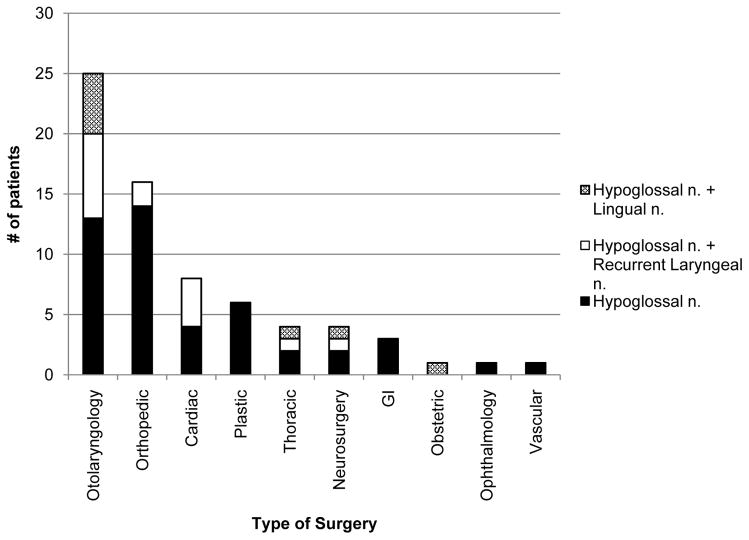
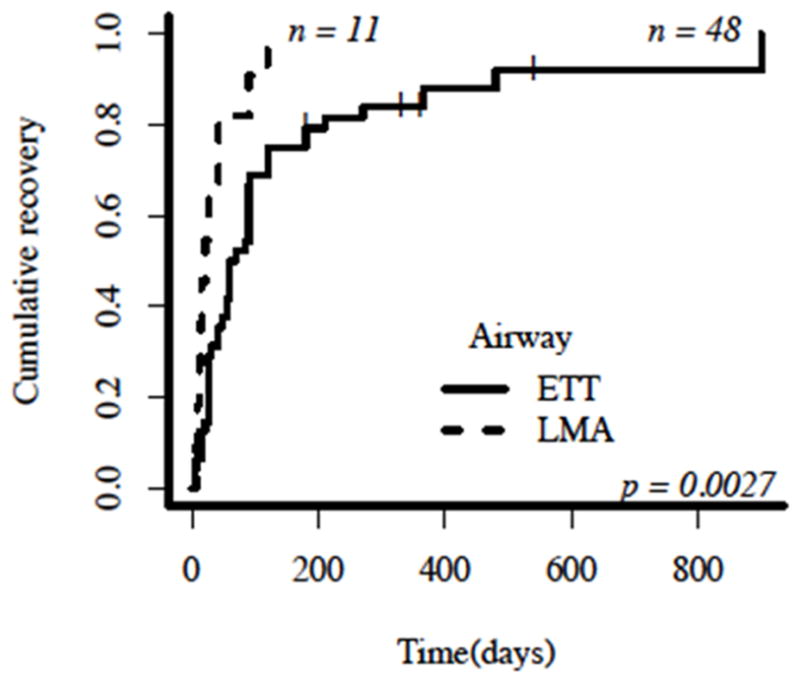
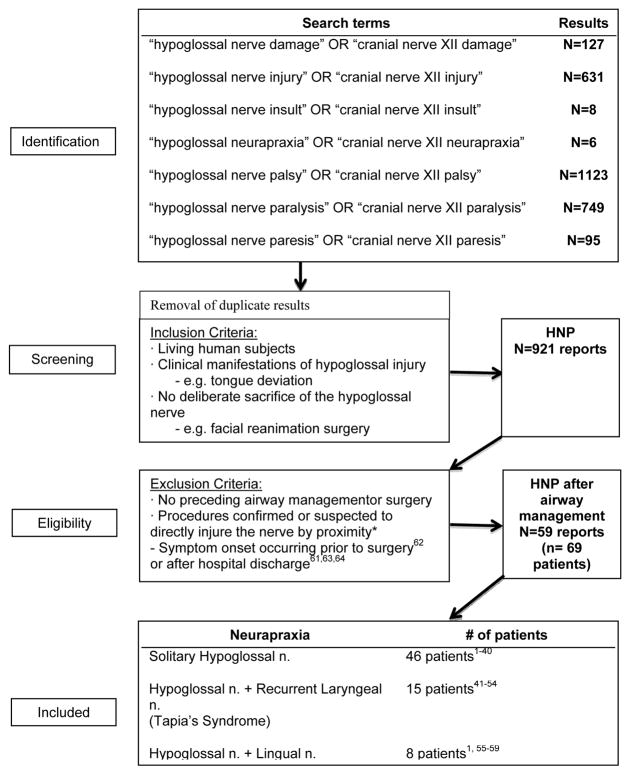
Isolated hypoglossal nerve palsy (HNP), or neurapraxia, a rare postoperative complication after airway management, causes ipsilateral tongue deviation, dysarthria, and dysphagia. We reviewed the pathophysiological causes of hypoglossal nerve injury and discuss the associated clinical and procedural characteristics of affected patients. Furthermore, we identified procedural factors potentially affecting HNP recovery duration and propose several measures that may reduce the risk of HNP. While HNP can occur after a variety of surgeries, most cases in the literature were reported after orthopedic and otolaryngology operations, typically in males. The diagnosis is frequently missed by the anesthesia care team in the recovery room due to the delayed symptomatic onset and often requires neurology and otolaryngology evaluations to exclude serious etiologies. Signs and symptoms are self-limited, with resolution occurring within 2 months in 50% of patients, and 80% resolving within 4 months. Currently, there are no specific preventive or therapeutic recommendations. We found 69 cases of HNP after procedural airway management reported in the literature from 1926 to 2013.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Agnoli A, Strauss P. Isolated paresis of hypoglossal nerve and combined paresis of hypoglossal nerve and lingual nerve following intubation and direct laryngoscopy. HNO. 1970;18:237–239. - PubMed
-
- Varedi P, Shirani G, Karimi A, Khiabani K, Bohluli B. Tapia syndrome after repairing a fractured zygomatic complex: A case report and review of the literature. J Oral Maxillofac Surg. 2013;71:1665–1669. - PubMed
-
- Baumgarten V, Jalinski W, Bohm S, Galle E. Hypoglossal paralysis after septum correction with intubation anesthesia. Anaesthesist. 1997;46:34–37. - PubMed
-
- Boenninghaus HG, Denecke U. Paralysis of the hypoglossal nerve after tonsillectomy? (author’s transl) Laryngol Rhinol Otol (Stuttg) 1982;61:189–192. - PubMed
-
- Boisseau N, Rabarijaona H, Grimaud D, Raucoules-Aime M. Tapia’s syndrome following shoulder surgery. Br J Anaesth. 2002;88:869–870. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
