

Enhancing aesthetic outcomes of soft-tissue coverage of the hand
- PMID: 25626826
- PMCID: PMC4789779
- DOI: 10.1097/PRS.0000000000001069
Enhancing aesthetic outcomes of soft-tissue coverage of the hand
Abstract
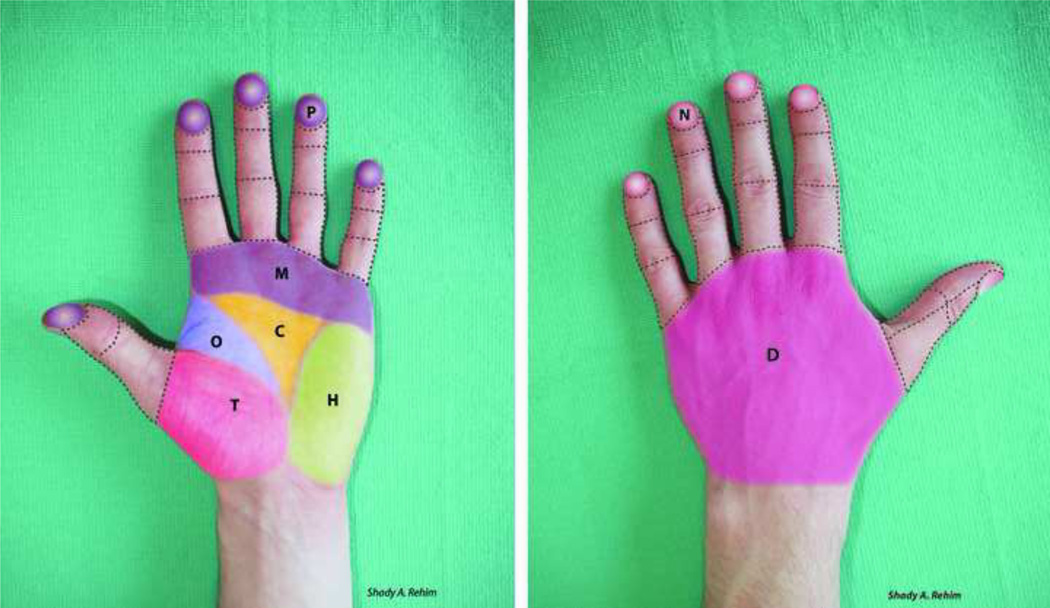
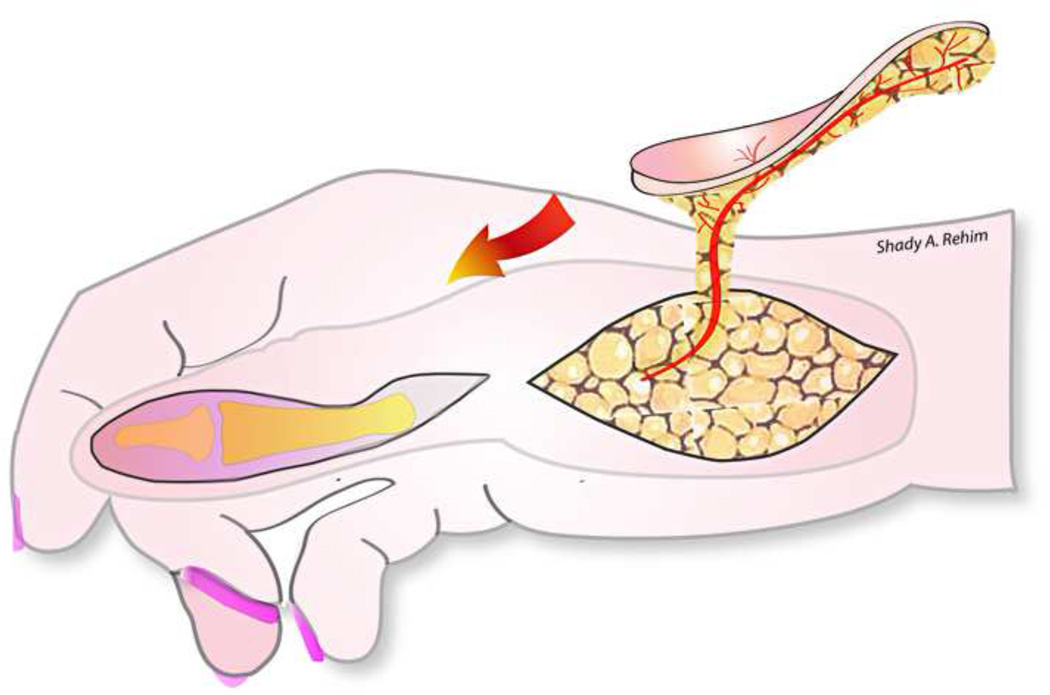
Hand aesthetics in general and aesthetic refinements of soft-tissue coverage of the hand in particular have been increasingly considered over the past few years. Advancements of microsurgery together with the traditional methods of tissue transfer have expanded the number of techniques available to the reconstructive surgeon, thus shifting the reconstructive paradigm from simply "filling the defect" to reconstructive refinement to provide the best functional and aesthetic results. However, drawing the boundary between what does and what does not constitute "aesthetic" reconstruction of the hand is not straightforward. The selection among the vast amount of currently available reconstructive methods and the difficulties in objectively measuring or quantifying aesthetics have made this task complex and rather arbitrary. In this article, the authors divide the hand into several units and subunits to simplify the understanding of the basic functional and aesthetic requirements of these regions that may ultimately bring order to complexity.
Figures







References
-
- McCash RC. Cosmetic aspects of hand surgery. The Hand. 1969 Mar;1(1):67–71.
-
- Manske PR. Aesthetic hand surgery. J Hand Surg Am. 2002;27:383–384. - PubMed
-
- Jakubietz RG, Jakubietz MG, Kloss D, Gruenert JG. Defining the Basic Aesthetics of the Hand. Aesthetic Plast Surg. 2005 Nov-Dec;29(6):546–551. - PubMed
-
- Rumsey N, Harcourt D. Body image and disfigurement: issues and interventions. Body Image. 2004 Jan;1(1):83–97. - PubMed
-
- Magee L. Traumatic Injuries and Body Image. Encyclopedia of Body Image and Human Appearance. 2012:790–797.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
