

Virological outcomes and treatment algorithms utilisation in observational study of patients with chronic hepatitis C treated with boceprevir or telaprevir
- PMID: 25627020
- PMCID: PMC4529024
- DOI: 10.1111/apt.13095
Virological outcomes and treatment algorithms utilisation in observational study of patients with chronic hepatitis C treated with boceprevir or telaprevir
Abstract
Background: HCV-TARGET is a longitudinal observational study of chronic hepatitis C virus (HCV) patients treated with direct-acting anti-viral agents (DAAs) in a US consortium of 90 academic and community medical centres.
Aim: To assess utilisation of response-guided therapy (RGT) and sustained virological response (SVR) of a large cohort of patients.
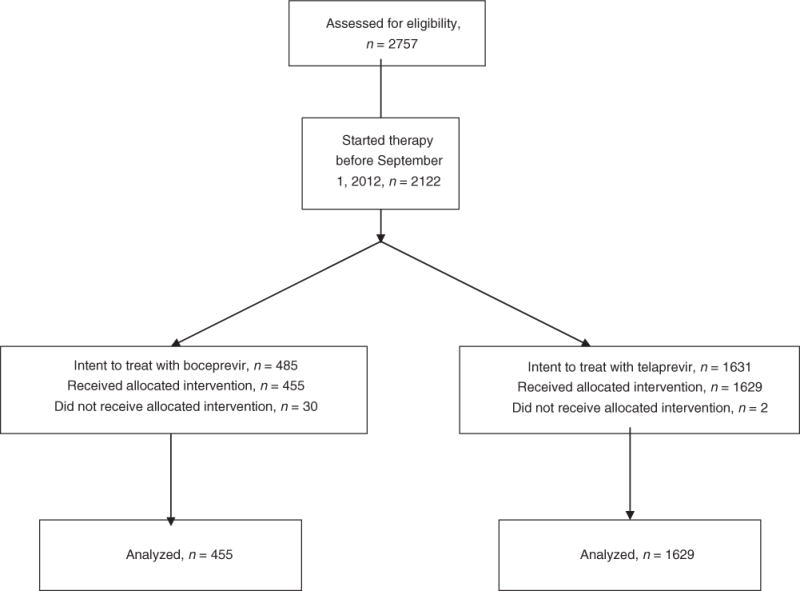
Methods: Patients received peginterferon (PEG-IFN), ribavirin and either telaprevir or boceprevir. Demographical, clinical and virological data were collected during treatment and follow-up. RGT and treatment futility stopping rules was assessed at key time points.
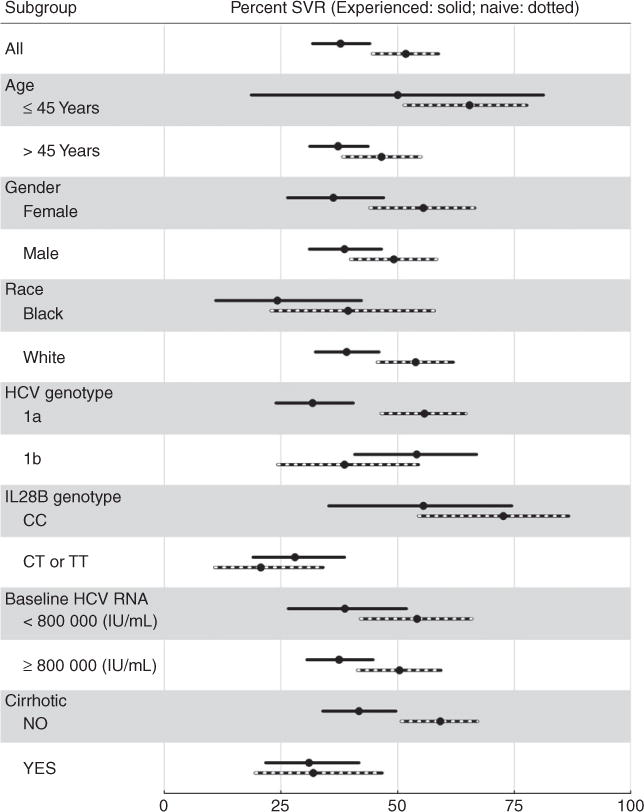
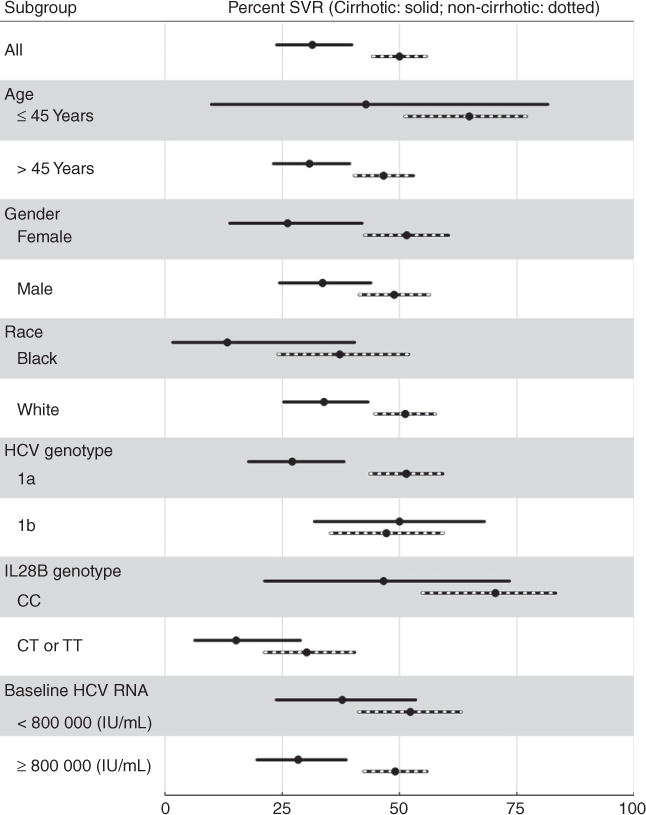
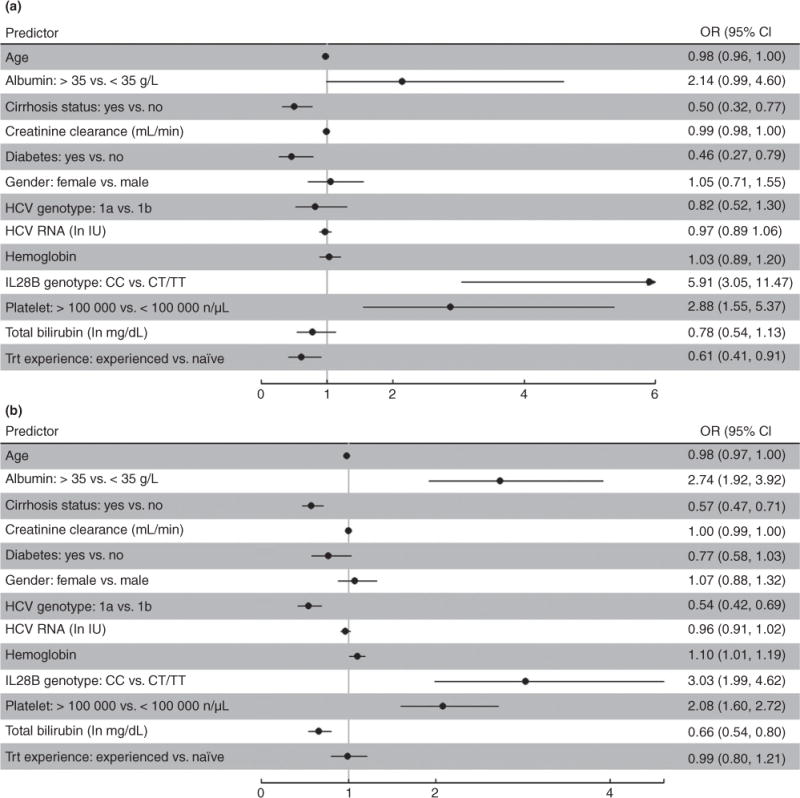
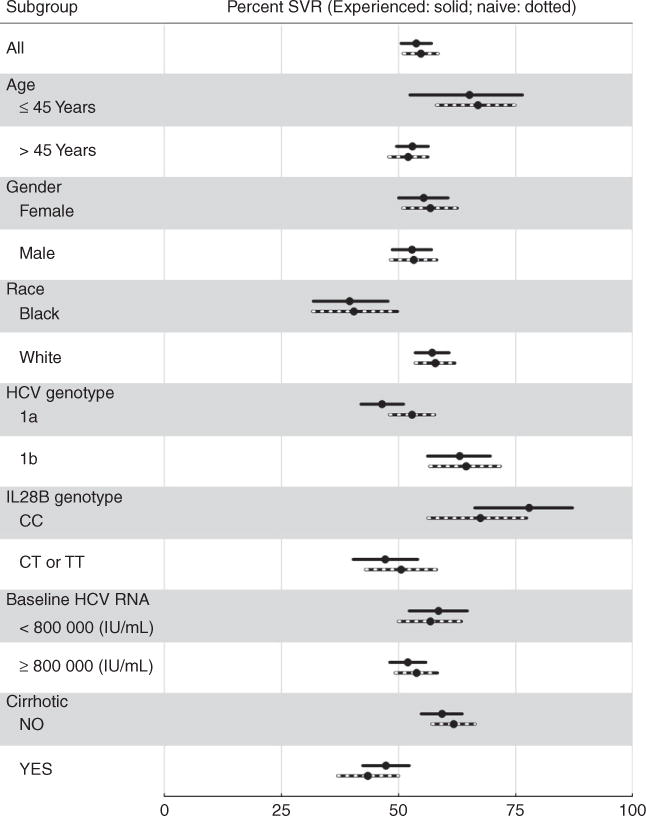
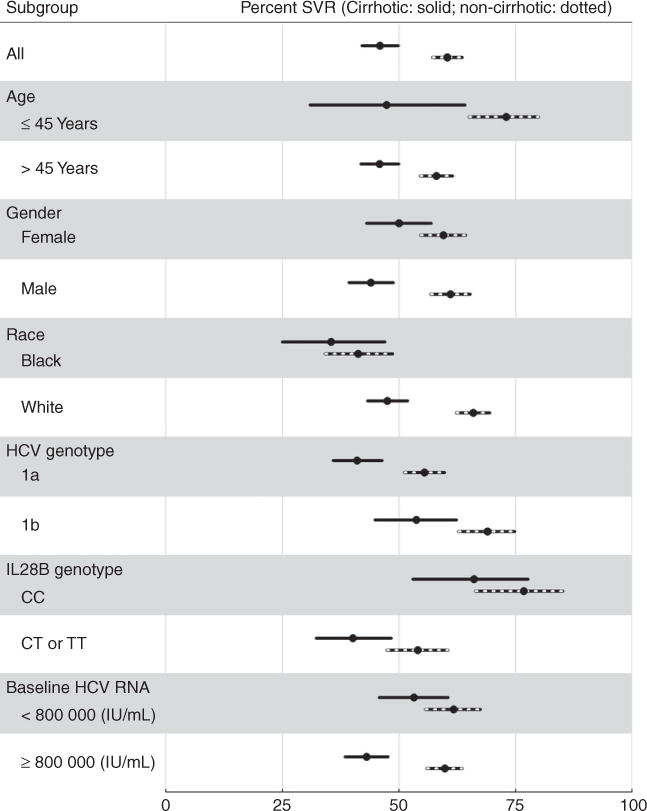
Results: Of 2084 patients, 38% had cirrhosis and 56% had received prior treatment for HCV. SVR rates were 31% (95% CI: 24-40) and 50% (95% CI: 44-56) in boceprevir patients with and without cirrhosis, respectively. SVR rates were 46% (95% CI: 42-50) and 60% (95% CI: 57-64) in telaprevir patients with and without cirrhosis, respectively. Early clearance of virus, IL28B genotype, platelet counts and diabetes were identified as predictors of SVR among boceprevir patients, while early clearance of virus, IL28B, cirrhosis, HCV subtype, age, haemoglobin, bilirubin and albumin levels were identified as predictors of SVR for telaprevir patients.
Conclusions: In academic and community centres, triple therapy including boceprevir or telaprevir led to SVR rates somewhat lower than those noted in large phase 3 clinical trials. Response rates were consistently higher among patients without cirrhosis compared to those with cirrhosis regardless of DAA used and prior treatment response. Trial registration clinicaltrials.gov NCT01474811.
© 2015 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
References
-
- Te HS, Jensen DM. Epidemiology of hepatitis B and C viruses: a global overview. Clin Liver Dis. 2010;14:1–21. vii. - PubMed
-
- Rustgi VK. The epidemiology of hepatitis C infection in the United States. J Gastroenterol. 2007;42:513–21. - PubMed
-
- Davis GL, Alter MJ, El-Serag H, Poynard T, Jennings LW. Aging of hepatitis C virus (HCV)-infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression. Gastroenterology. 2010;138:513–21. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical