

Cost-effectiveness of strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in an intensive care unit
- PMID: 25627757
- PMCID: PMC4311265
- DOI: 10.1017/ice.2014.12
Cost-effectiveness of strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in an intensive care unit
Abstract
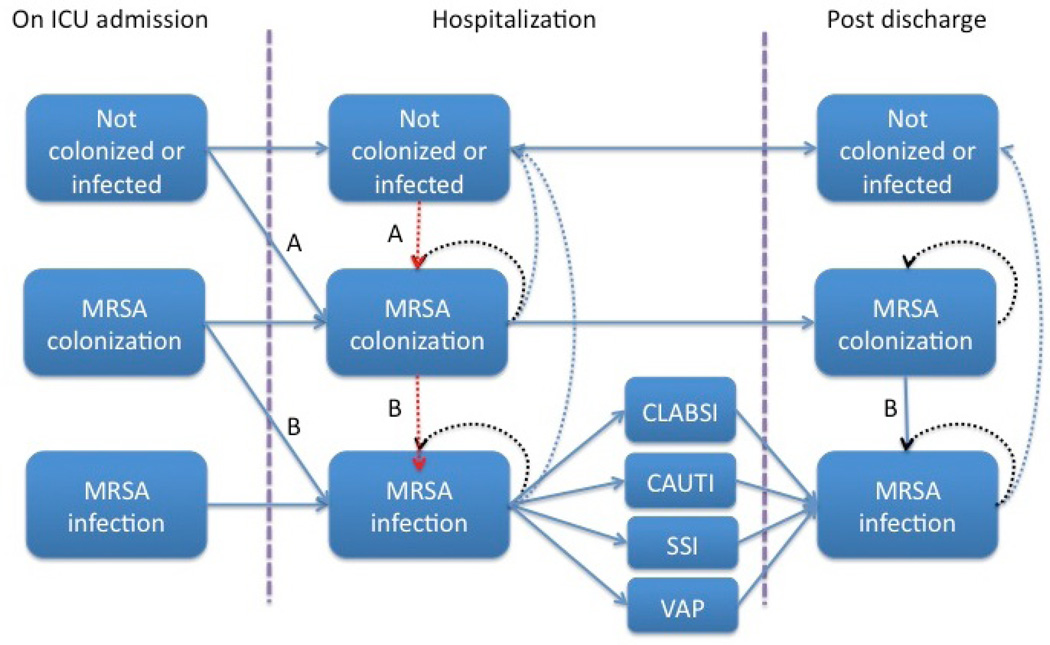
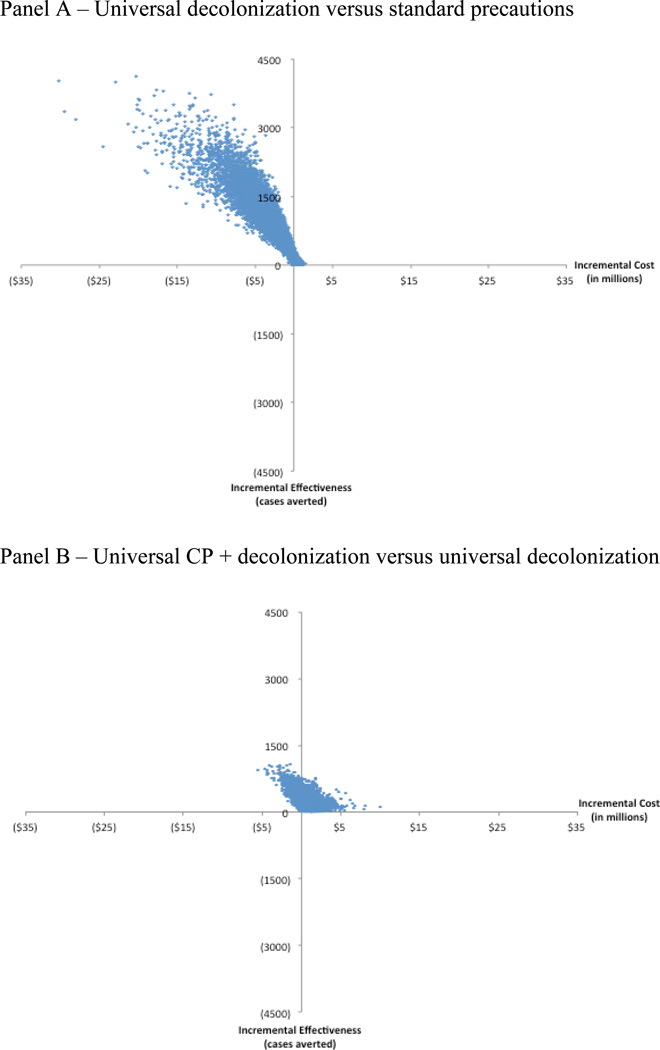
OBJECTIVE To create a national policy model to evaluate the projected cost-effectiveness of multiple hospital-based strategies to prevent methicillin-resistant Staphylococcus aureus (MRSA) transmission and infection. DESIGN Cost-effectiveness analysis using a Markov microsimulation model that simulates the natural history of MRSA acquisition and infection. PATIENTS AND SETTING Hypothetical cohort of 10,000 adult patients admitted to a US intensive care unit. METHODS We compared 7 strategies to standard precautions using a hospital perspective: (1) active surveillance cultures; (2) active surveillance cultures plus selective decolonization; (3) universal contact precautions (UCP); (4) universal chlorhexidine gluconate baths; (5) universal decolonization; (6) UCP + chlorhexidine gluconate baths; and (7) UCP+decolonization. For each strategy, both efficacy and compliance were considered. Outcomes of interest were: (1) MRSA colonization averted; (2) MRSA infection averted; (3) incremental cost per colonization averted; (4) incremental cost per infection averted. RESULTS A total of 1989 cases of colonization and 544 MRSA invasive infections occurred under standard precautions per 10,000 patients. Universal decolonization was the least expensive strategy and was more effective compared with all strategies except UCP+decolonization and UCP+chlorhexidine gluconate. UCP+decolonization was more effective than universal decolonization but would cost $2469 per colonization averted and $9007 per infection averted. If MRSA colonization prevalence decreases from 12% to 5%, active surveillance cultures plus selective decolonization becomes the least expensive strategy. CONCLUSIONS Universal decolonization is cost-saving, preventing 44% of cases of MRSA colonization and 45% of cases of MRSA infection. Our model provides useful guidance for decision makers choosing between multiple available hospital-based strategies to prevent MRSA transmission.
Conflict of interest statement
The remaining authors have no conflict of interest to report.
Figures

Similar articles
-
Methicillin-resistant Staphylococcus aureus prevention strategies in the ICU: a clinical decision analysis*.Crit Care Med. 2015 Feb;43(2):382-93. doi: 10.1097/CCM.0000000000000711. Crit Care Med. 2015. PMID: 25377019
-
Impact of active screening for methicillin-resistant Staphylococcus aureus (MRSA) and decolonization on MRSA infections, mortality and medical cost: a quasi-experimental study in surgical intensive care unit.Crit Care. 2015 Apr 8;19(1):143. doi: 10.1186/s13054-015-0876-y. Crit Care. 2015. PMID: 25882709 Free PMC article.
-
Agents for the decolonization of methicillin-resistant Staphylococcus aureus.Pharmacotherapy. 2009 Mar;29(3):263-80. doi: 10.1592/phco.29.3.263. Pharmacotherapy. 2009. PMID: 19249946 Review.
-
Has decolonization played a central role in the decline in UK methicillin-resistant Staphylococcus aureus transmission? A focus on evidence from intensive care.J Antimicrob Chemother. 2011 Apr;66 Suppl 2:ii41-7. doi: 10.1093/jac/dkq325. Epub 2010 Sep 18. J Antimicrob Chemother. 2011. PMID: 20852273 Review.
-
Recommendations for Methicillin-Resistant Staphylococcus aureus Prevention in Adult ICUs: A Cost-Effectiveness Analysis.Crit Care Med. 2017 Aug;45(8):1304-1310. doi: 10.1097/CCM.0000000000002484. Crit Care Med. 2017. PMID: 28471887
Cited by
-
Staphylococcus aureus with reduced susceptibility to vancomycin in healthcare settings.J Prev Med Hyg. 2014 Dec;55(4):137-44. J Prev Med Hyg. 2014. PMID: 26137787 Free PMC article. Review.
-
Staphylococcus aureus in the Intensive Care Unit: Are These Golden Grapes Ripe for a New Approach?J Infect Dis. 2017 Feb 15;215(suppl_1):S64-S70. doi: 10.1093/infdis/jiw581. J Infect Dis. 2017. PMID: 28003353 Free PMC article. Review.
-
Analysis of the dynamics of transition from non-colonization to colonization and Staphylococcus aureus bacteremia in hemodialysis patients using Markov models.F1000Res. 2025 Jan 6;13:837. doi: 10.12688/f1000research.151896.3. eCollection 2024. F1000Res. 2025. PMID: 39931330 Free PMC article.
-
Economic Evaluation of Interventions to Reduce Antimicrobial Resistance: A Systematic Literature Review of Methods.Pharmacoeconomics. 2025 Jun;43(6):631-646. doi: 10.1007/s40273-024-01468-7. Epub 2025 Mar 6. Pharmacoeconomics. 2025. PMID: 40048093
-
Methicillin-Resistant Staphylococcus aureus Colonization in Intensive Care and Burn Units: A Narrative Review.Cureus. 2023 Oct 16;15(10):e47139. doi: 10.7759/cureus.47139. eCollection 2023 Oct. Cureus. 2023. PMID: 38021721 Free PMC article. Review.
References
-
- National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32:470–485. - PubMed
-
- Huang SS, Platt R. Risk of methicillin-resistant Staphylococcus aureus infection after previous infection or colonization. Clin Infect Dis. 2003;36:281–285. - PubMed
-
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36:53–59. - PubMed
-
- Engemann JJ, Carmeli Y, Cosgrove SE, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis. 2003;36:592–598. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
