

PART is part of Alzheimer disease
- PMID: 25628035
- PMCID: PMC4405349
- DOI: 10.1007/s00401-015-1390-7
PART is part of Alzheimer disease
Abstract
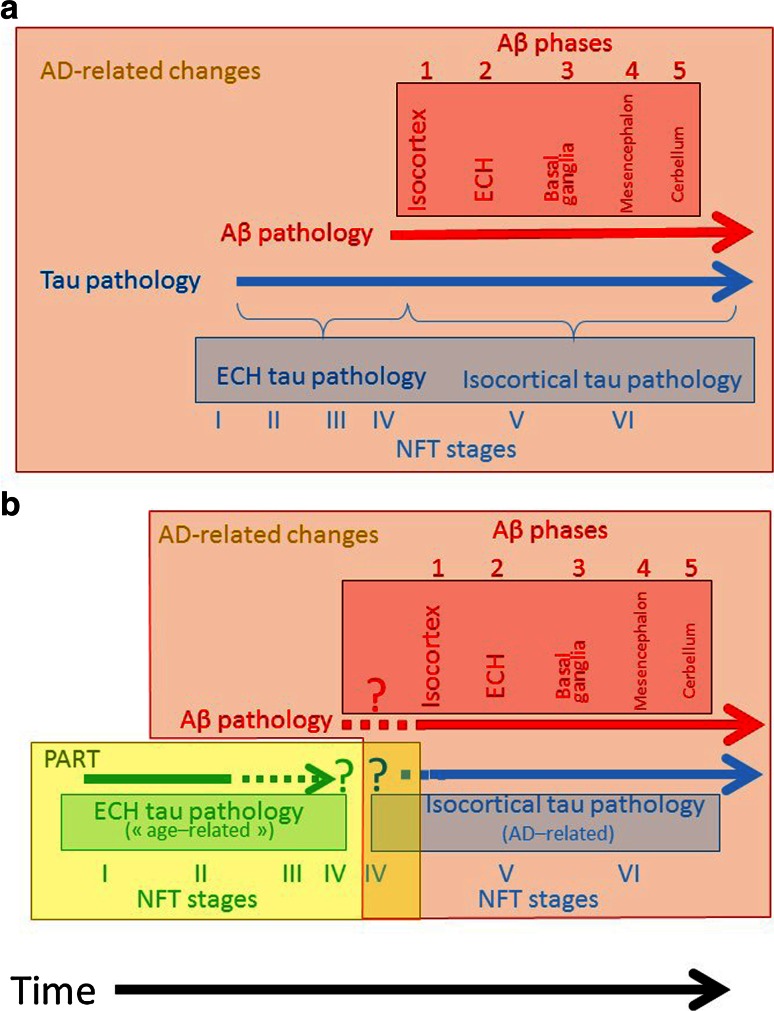
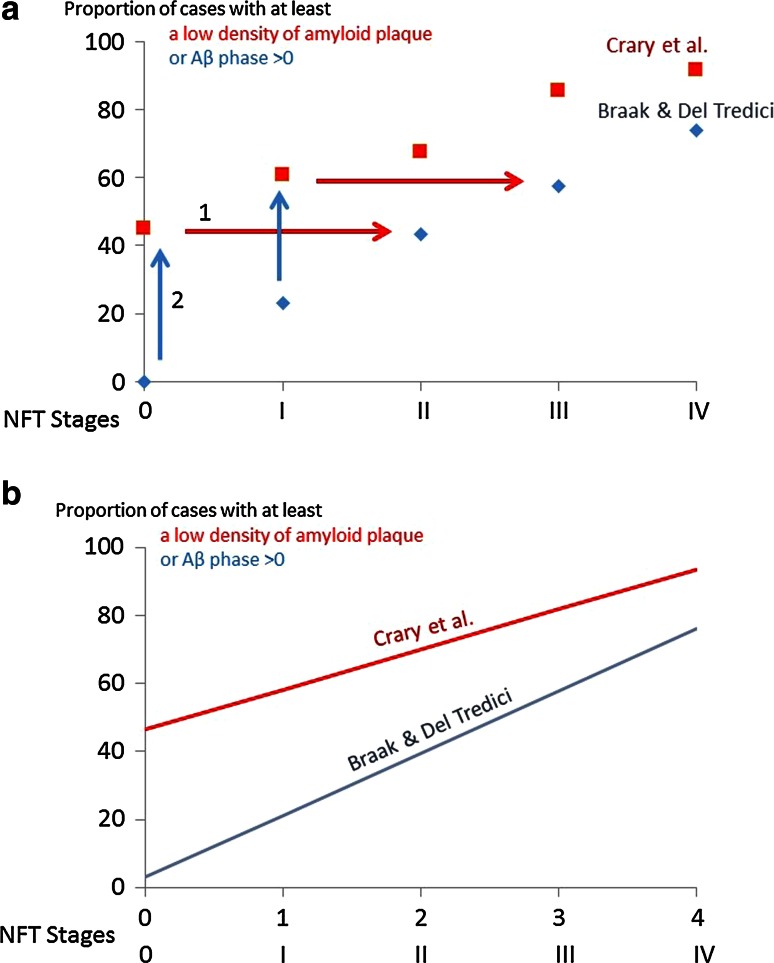
It has been proposed that tau aggregation confined to entorhinal cortex and hippocampus, with no or only minimal Aβ deposition, should be considered as a 'primary age-related tauopathy' (PART) that is not integral to the continuum of sporadic Alzheimer disease (AD). Here, we examine the evidence that PART has a pathogenic mechanism and a prognosis which differ from those of AD. We contend that no specific property of the entorhinal-hippocampal tau pathology makes it possible to predict either a limited progression or the development of AD, and that biochemical differences await an evidence base. On the other hand, entorhinal-hippocampal tau pathology is an invariant feature of AD and is always associated with its development. Rather than creating a separate disease entity, we recommend the continued use of an analytical approach based on NFT stages and Aβ phases with no inference about hypothetical disease processes.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
