

Histology subtypes and polyp size are associated with synchronous colorectal carcinoma of colorectal serrated polyps: a study of 499 serrated polyps
- PMID: 25628945
- PMCID: PMC4300721
Histology subtypes and polyp size are associated with synchronous colorectal carcinoma of colorectal serrated polyps: a study of 499 serrated polyps
Abstract
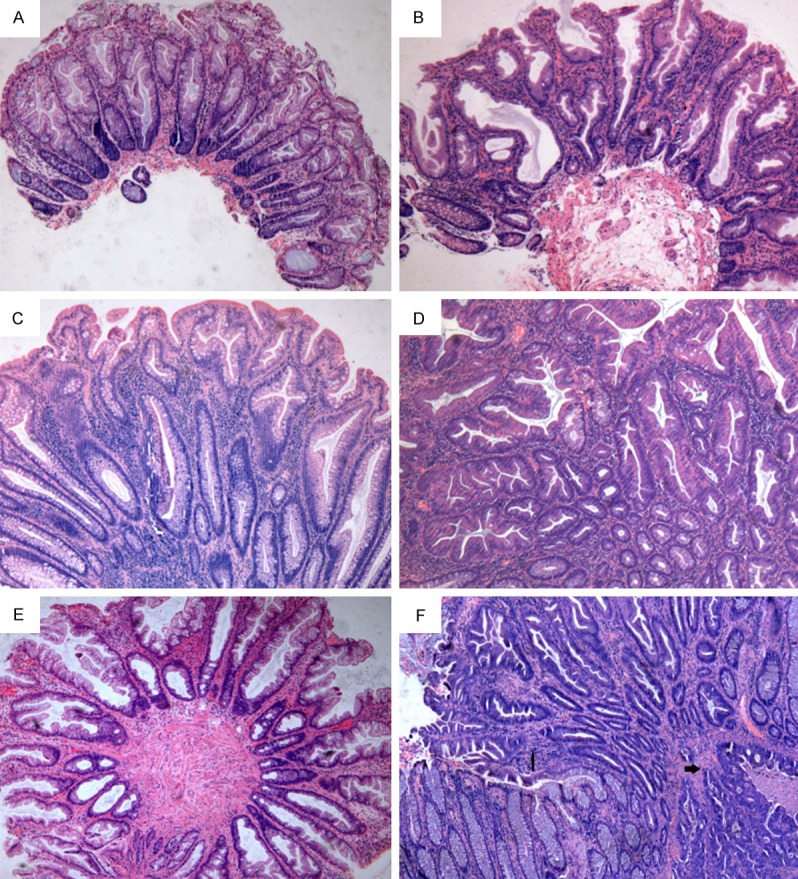
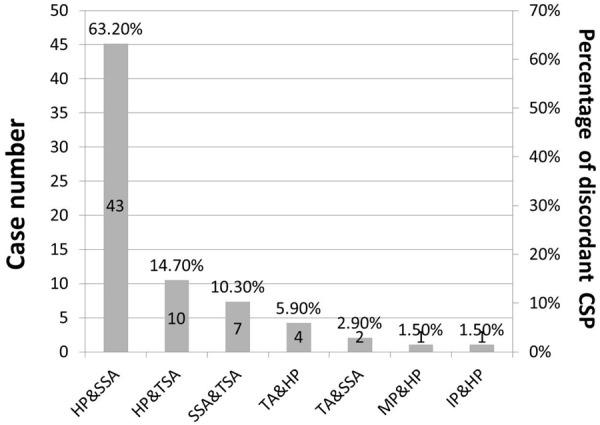
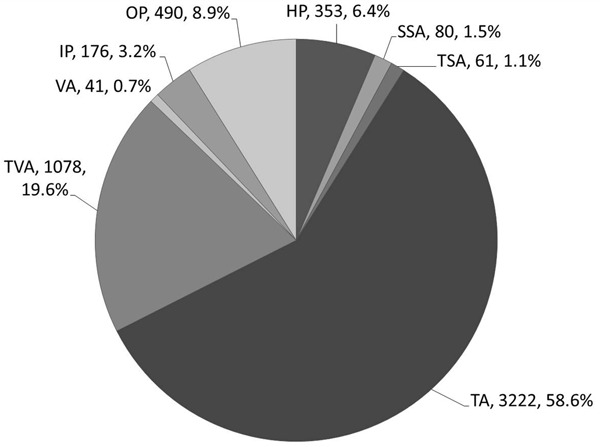
Sessile serrated adenomas (SSA) and traditional serrated adenomas (TSA) are considered as precursors of colorectal cancer, and are often diagnostic challenges. Their true prevalence is masked by significant inter-observer variations. To investigate the true prevalence and synchronous colorectal carcinoma (sCRC) of colorectal serrated polyps (CSP) and their associated factors, we first retrospectively identified all colorectal polyps collected at our institution between June 1995 and May 2013. After centrally reclassifying all CSP to reduce inter-observer variations, Chi-square tests and logistic regression analyses were used to analyze the potential factors. Among the included 5501 colorectal polyps, 499 CSP of 428 patients were identified and studied, including 353 hyperplastic polyps (HP, 70.7%), 80 SSA (16.0%), 61 TSA (12.2%) and 5 mixed polyp (1.0%). Diagnostic disagreements were found in 68 CSP (13.63% of CSP). SSA and TSA were more often larger than 5 mm and in proximal colon than HP. SSA were also more likely associated with older age (p=0.005), size ≥5 mm (p<0.001) and ≥3 polyps (p=0.004) than HP in distal colon, but only more likely associated with older age (p=0.006) in proximal colon. Multivariate regression analysis demonstrated that CSP with sCRC, compared with CSP without sCRC, were linked to CSP size ≥1 cm (vs <1 cm, odds ratio [OR] 4.412, 95% confidence interval [CI] 1.684-11.556, P=0.003) and a diagnosis of SSA or TSA (vs HP, OR 6.194, 95% CI 1.870-20.513, P=0.003 and OR 6.754, 95% CI 1.981-23.028, P=0.002, respectively), but not age, gender, polyp number and polyp shape. SSA and TSA are similarly often associated with sCRC (P=0.460). In conclusion, histology subtypes and polyp size may serve as markers for sCRC of CSP. SSA and TSA may warrant careful endoscopic examinations and similar follow-up intervals.
Keywords: Conventional adenoma; colon; hyperplastic polyp; sessile serrated adenoma; traditional serrated adenoma.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Shaukat A, Mongin SJ, Geisser MS, Lederle FA, Bond JH, Mandel JS, Church TR. Long-term mortality after screening for colorectal cancer. N Engl J Med. 2013;369:1106–1114. - PubMed
-
- le Clercq CM, Bouwens MW, Rondagh EJ, Bakker CM, Keulen ET, de Ridder RJ, Winkens B, Masclee AA, Sanduleanu S. Postcolonoscopy colorectal cancers are preventable: a population-based study. Gut. 2014;63:957–963. - PubMed
-
- Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Gottlieb LS, Sternberg SS, Waye JD, Schapiro M, Bond JH, Panish JF, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981. - PubMed
-
- Lieberman DA American Gastroenterological Association. Colon polyp surveillance: clinical decision tool. Gastroenterology. 2014;146:305–306. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous