

Characteristics of Circulating Donor Human Leukocyte Antigen-specific Immunoglobulin G Antibodies Predictive of Acute Antibody-mediated Rejection and Kidney Allograft Failure
- PMID: 25629531
- PMCID: PMC4729299
- DOI: 10.1097/TP.0000000000000511
Characteristics of Circulating Donor Human Leukocyte Antigen-specific Immunoglobulin G Antibodies Predictive of Acute Antibody-mediated Rejection and Kidney Allograft Failure
Abstract
Background: Characteristics of pretransplant antibodies directed at donor human leukocyte antigen (HLA) donor-specific antibodies (DSA) associated with adverse outcomes in kidney transplant recipients are being elucidated but uncertainties exist.
Methods: We prospectively screened pretransplant sera from 543 kidney recipients using single antigen bead assays and identified 154 patients with and 389 without DSA. We investigated the association of DSA features to acute rejection and graft failure.
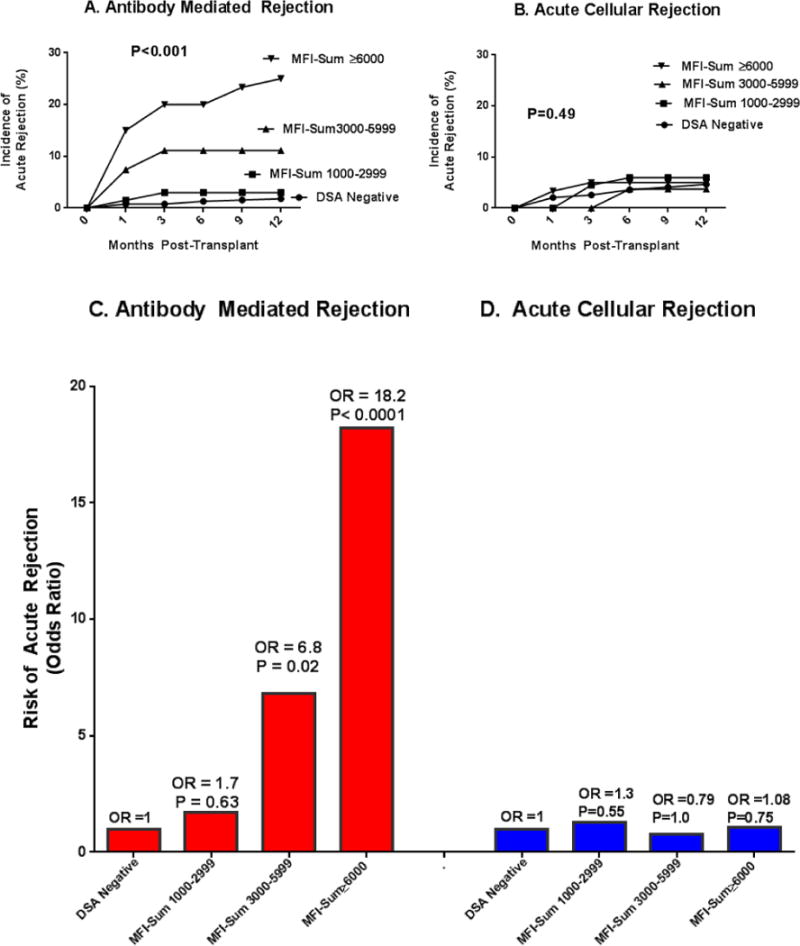
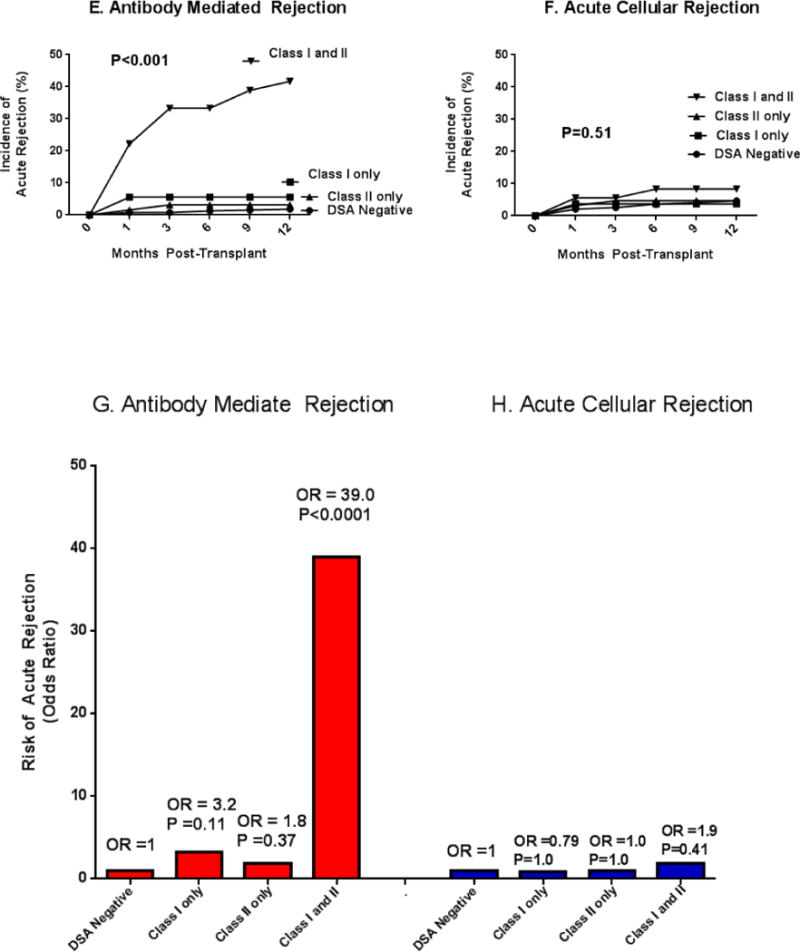
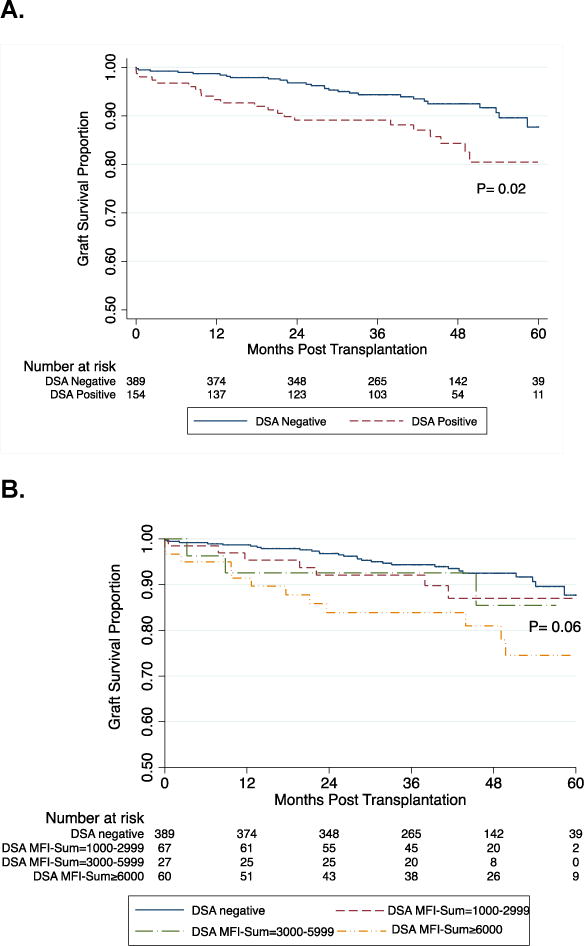
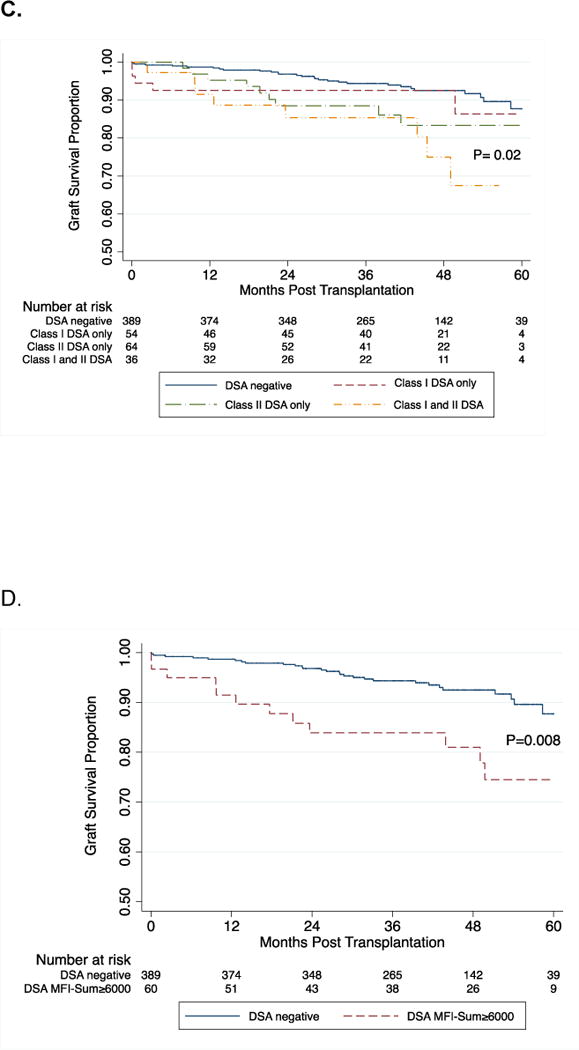
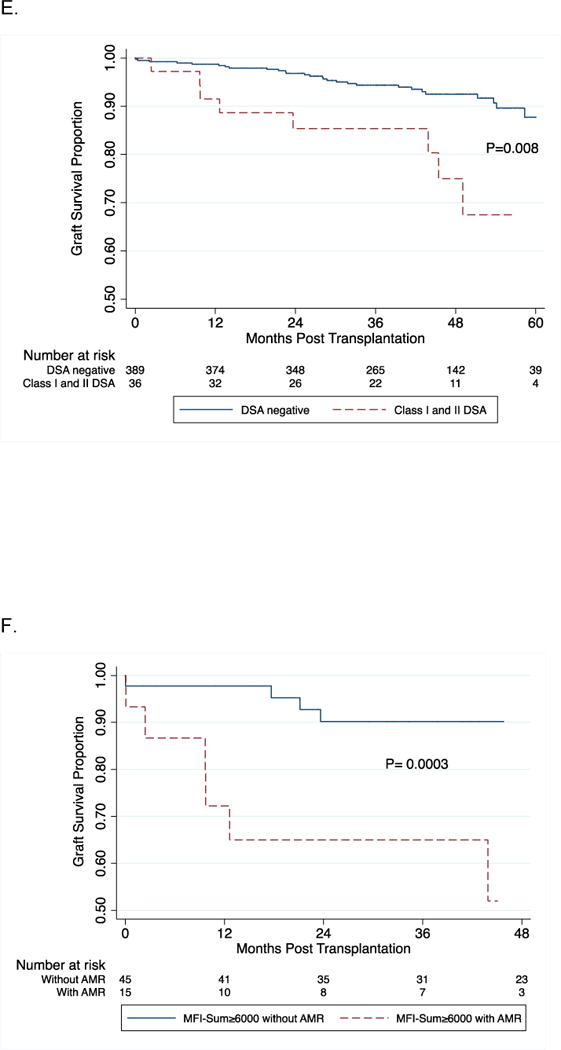
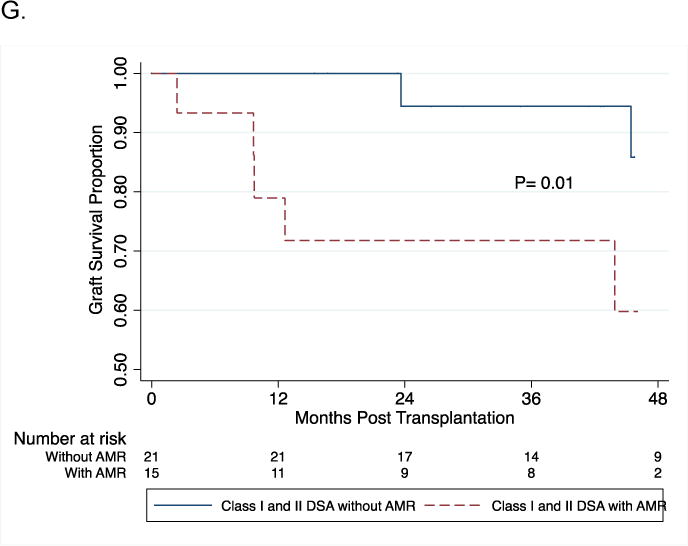
Results: One-year acute rejection incidence was higher in DSA-positive group (P < 0.001), primarily due to antibody-mediated rejection (AMR, 13% vs. 1.8%, P < 0.001) and not T cell-mediated rejection (ACR, 5% vs.6%, P = 0.65). The sum of mean fluorescence intensity of DSA (DSA MFI-Sum) of 6,000 or higher (OR, 18; 95% CI, 7.0-47; P < 0.001) and the presence of DSA against both HLA class I and II (OR, 39; 95% CI, 14-106; P < 0.0001) predicted 1-year AMR, independent of other covariates. Calculated panel reactive antibody and a positive flow cytometry cross-match result were associated with AMR by bivariate analysis but neither was an independent predictor in a multivariable regression analysis that included DSA-MFI-Sum or HLA DSA class. In multivariable Cox proportional hazards models, the covariate-adjusted hazard ratio for graft failure was 2.03 (95%CI, 1.05-3.92; P = 0.04) for DSA MFI-Sum of 6,000 or higher and 2.23 (95% CI, 1.04-4.80; P = 0.04) for class I and II DSA. Prediction of graft failure was not independent of AMR.
Conclusion: Our study suggests that DSA MFI-Sum and HLA class of DSA are characteristics predictive of AMR and graft failure. The elevated risk of graft failure in those with the identified features of DSA is attributable to increased risk of AMR.
Figures
References
-
- Patel R, Terasaki PI. Significance of the positive crossmatch test in kidney transplantation. The New England journal of medicine. 1969;280(14):735–9. - PubMed
-
- Ozawa M, Terasaki PI, Castro R, Alberu J, Morales-Buenrostro L, Alvarez I, et al. 14th International HLA and Immunogenetics Workshop Prospective Chronic Rejection Project: a three-year follow-up analysis. Clinical transplants. 2007:255–60. - PubMed
-
- Lefaucheur C, Suberbielle-Boissel C, Hill GS, Nochy D, Andrade J, Antoine C, et al. Clinical relevance of preformed HLA donor-specific antibodies in kidney transplantation. American journal of transplantation: official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2008;8(2):324–31. - PubMed
-
- Gibney EM, Cagle LR, Freed B, Warnell SE, Chan L, Wiseman AC. Detection of donor-specific antibodies using HLA-coated microspheres: another tool for kidney transplant risk stratification. Nephrology, dialysis, transplantation: official publication of the European Dialysis and Transplant Association - European Renal Association. 2006;21(9):2625–9. - PubMed
-
- Pei R, Lee J, Chen T, Rojo S, Terasaki PI. Flow cytometric detection of HLA antibodies using a spectrum of microbeads. Human immunology. 1999;60(12):1293–302. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
