

Cardiotoxicity during invasive pneumococcal disease
- PMID: 25629643
- PMCID: PMC4407487
- DOI: 10.1164/rccm.201411-1951PP
Cardiotoxicity during invasive pneumococcal disease
Abstract
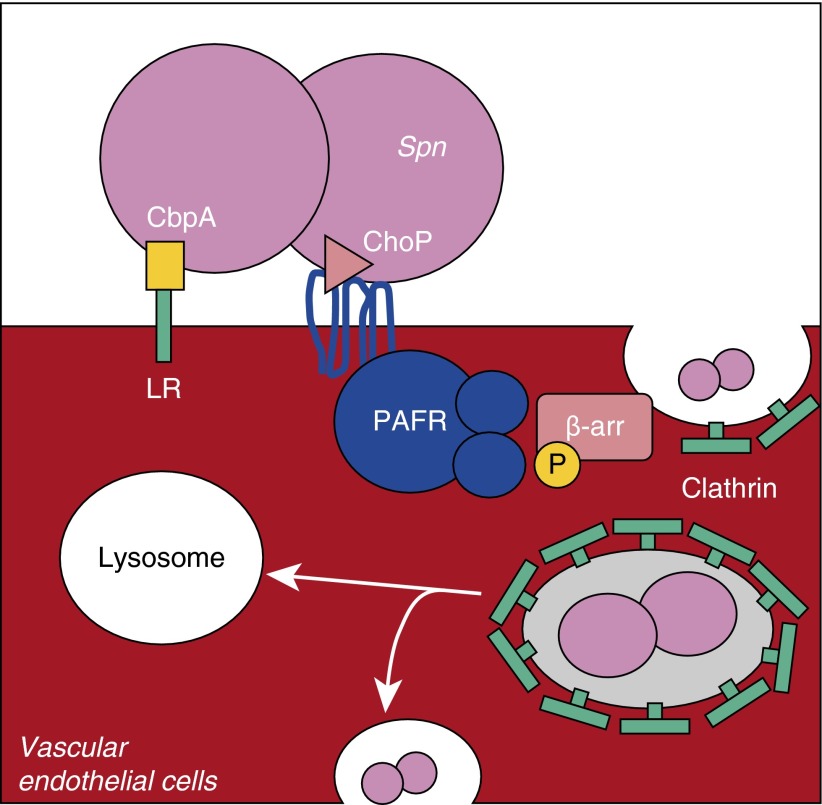
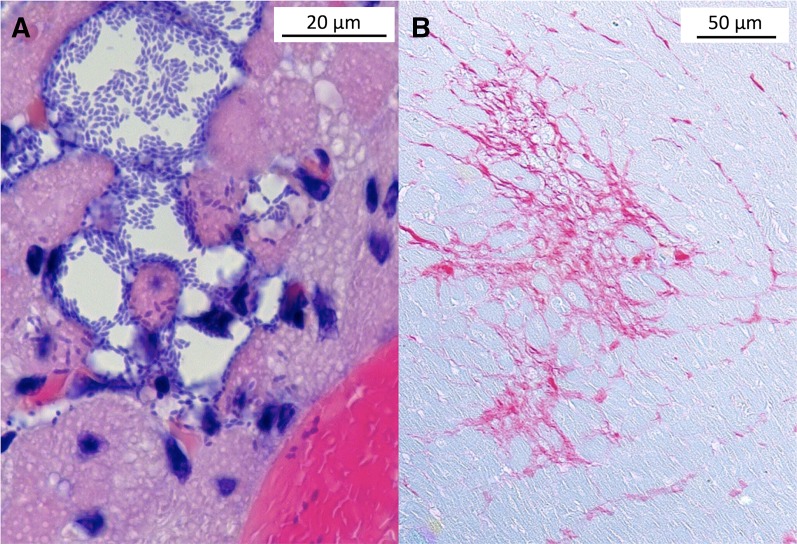
Streptococcus pneumoniae is the leading cause of community-acquired pneumonia and sepsis, with adult hospitalization linked to approximately 19% incidence of an adverse cardiac event (e.g., heart failure, arrhythmia, infarction). Herein, we review the specific host-pathogen interactions that contribute to cardiac dysfunction during invasive pneumococcal disease: (1) cell wall-mediated inhibition of cardiomyocyte contractility; (2) the new observation that S. pneumoniae is capable of translocation into the myocardium and within the heart, forming discrete, nonpurulent, microscopic lesions that are filled with pneumococci; and (3) the bacterial virulence determinants, pneumolysin and hydrogen peroxide, that are most likely responsible for cardiomyocyte cell death. Pneumococcal invasion of heart tissue is dependent on the bacterial adhesin choline-binding protein A that binds to laminin receptor on vascular endothelial cells and binding of phosphorylcholine residues on pneumococcal cell wall to platelet-activating factor receptor. These are the same interactions responsible for pneumococcal translocation across the blood-brain barrier during the development of meningitis. We discuss these interactions and how their neutralization, either with antibody or therapeutic agents that modulate platelet-activating factor receptor expression, may confer protection against cardiac damage and meningitis. Considerable collagen deposition was observed in hearts of mice that had recovered from invasive pneumococcal disease. We discuss the possibility that cardiac scar formation after severe pneumococcal infection may explain why individuals who are hospitalized for pneumonia are at greater risk for sudden death up to 1 year after infection.
Keywords: Streptococcus pneumoniae; heart failure; invasion; invasive pneumococcal disease; pathogenesis.
Figures
References
-
- (UNICEF) UNCsFCommitting to child survival: a promise renewed. New York: United Nations; 2013. Progress report no. 978-92-806-4706-8
-
- European Respiratory Society. Sheffield, UK: ERS; 2015. European lung white book.
-
- File TM, Jr, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med. 2010;122:130–141. - PubMed
-
- Hoyert DL, Xu JQ. Hyattsville, MD: National Center for Health Statistics; 2012. Deaths: preliminary data for 2011. - PubMed
