

Review
doi: 10.1056/NEJMcp1412282.
Clinical practice. Allergic rhinitis
- PMID: 25629743
- PMCID: PMC4324099
- DOI: 10.1056/NEJMcp1412282
Item in Clipboard
Review
Clinical practice. Allergic rhinitis
N Engl J Med.
.
Abstract
A 35-year-old woman has a history of nasal congestion on most days of the year, dating back to her late teens. She has chronic nasal drainage, which is clear and thick. Her congestion is worst in the late summer and early fall and again in the early spring; at these times, she also has sneezing, nasal itching, and cough. Five years ago, she had an episode of shortness of breath with wheezing on a day when her nasal symptoms were severe, but this episode resolved spontaneously and has not recurred. Her eyes do not bother her. Over-the-counter oral antihistamines help her symptoms a little, as do nasal decongestants, which she uses occasionally. Her 6-year-old son has similar symptoms. How should this case be managed?
Figures
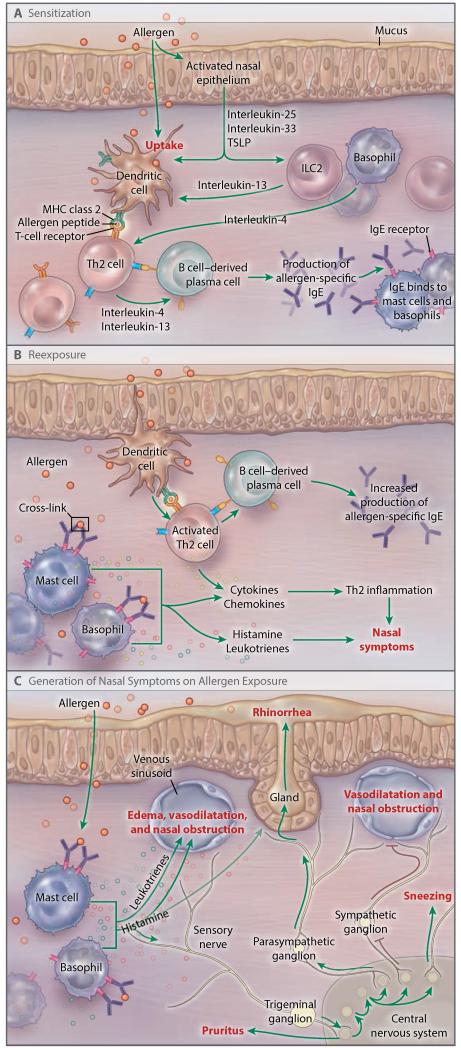
As shown in Panel A, sensitization involves allergen uptake by antigen-presenting cells (dendritic cells) at a mucosal site, leading to activation of antigen-specific T cells, most likely at draining lymph nodes. Simultaneous activation of epithelial cells by nonantigenic pathways (e.g., proteases) can lead to the release of epithelial cytokines (thymic stromal lymphopoietin [TSLP], interleukin-25, and interleukin-33), which can polarize the sensitization process into a type 2 helper T (Th2) cell response. This polarization is directed toward the dendritic cells and probably involves the participation of type 2 innate lymphoid cells (ILC2) and basophils, which release Th2-driving cytokines (interleukin-13 and interleukin-4). The result of this process is the generation of Th2 cells, which, in turn, drive B cells to become allergen-specific IgE-producing plasma cells. MHC denotes major histocompatibility complex. As shown in Panel B, allergen-specific IgE antibodies attach to high-affinity receptors on the surface of tissue-resident mast cells and circulating basophils. On reexposure, the allergen binds to IgE on the surface of those cells and cross-links IgE receptors, resulting in mast-cell and basophil activation and the release of neuroactive and vasoactive mediators such as histamine and the cysteinyl leukotrienes. These substances produce the typical symptoms of allergic rhinitis. In addition, local activation of Th2 lymphocytes by dendritic cells results in the release of chemokines and cytokines that orchestrate the influx of inflammatory cells (eosinophils, basophils, neutrophils, T cells, and B cells) to the mucosa, providing more allergen targets and up-regulating the end organs of the nose (nerves, vasculature, and glands). Th2 inflammation renders the nasal mucosa more sensitive to allergen but also to environmental irritants. In addition, exposure to allergen further stimulates production of IgE. As shown in Panel C, mediators released by mast cells and basophils can directly activate sensory-nerve endings, blood vessels, and glands through specific receptors. Histamine seems to have direct effects on blood vessels (leading to vascular permeability and plasma leakage) and sensory nerves, whereas leukotrienes are more likely to cause vasodilatation. Activation of sensory nerves leads to the generation of pruritus and to various central reflexes. These include a motor reflex leading to sneezing and parasympathetic reflexes that stimulate nasal-gland secretion and produce some vasodilatation. In addition, the sympathetic drive to the erectile venous sinusoids of the nose is suppressed, allowing for vascular engorgement and obstruction of the nasal passages. In the presence of allergic inflammation, these end-organ responses become up-regulated and more pronounced. Sensory-nerve hyperresponsiveness is a common pathophysiological feature of allergic rhinitis.
References
-
- Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen) Allergy. 2008;63(Suppl 86):8–160. - PubMed
-
- Yonekura S, Okamoto Y, Horiguchi S, et al. Effects of aging on the natural history of seasonal allergic rhinitis in middle-aged subjects in South Chiba, Japan. Int Arch Allergy Immunol. 2012;157:73–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical