

Laparoscopic Versus Open Gastrectomy for Gastric Adenocarcinoma in the West: A Case-Control Study
- PMID: 25631063
- PMCID: PMC5050554
- DOI: 10.1245/s10434-015-4381-y
Laparoscopic Versus Open Gastrectomy for Gastric Adenocarcinoma in the West: A Case-Control Study
Abstract
Introduction: Data on laparoscopic gastrectomy in patients with gastric cancer in the Western hemisphere are lacking. This study aimed to compare outcomes following laparoscopic versus open gastrectomy for gastric adenocarcinoma at a Western center.
Methods: Eighty-seven consecutive patients who underwent laparoscopic gastrectomy from November 2005 to April 2013 were compared with 87 patients undergoing open resection during the same time period. Patients were matched for age, stage, body mass index, and procedure (distal subtotal vs. total gastrectomy). Endpoints were short- and long-term perioperative outcomes.
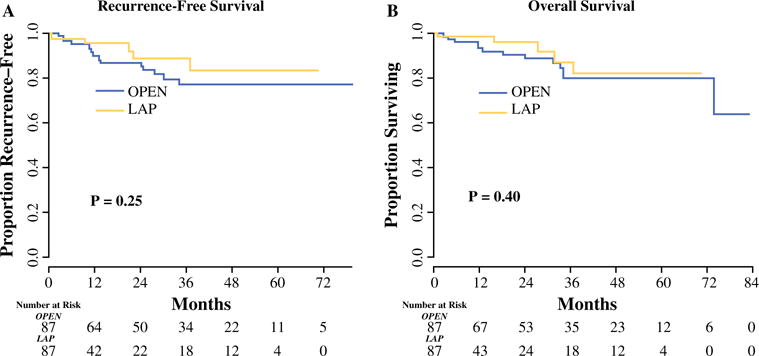
Results: Overall, 65 patients (37 %) had locally advanced disease, and 40 (23 %) had proximal tumors. The laparoscopic approach was associated with longer operative time (median 240 vs.165 min; p < 0.01), less blood loss (100 vs.150 mL; p < 0.01), higher rate of microscopic margin positivity (9 vs.1 %; p = 0.04), decreased duration of narcotic and epidural use (2 vs. 4 days, p = 0.04, and 3 vs. 4 days, p = 0.02, respectively), decreased minor complications in the early (27 vs. 16 %) and late (17 vs. 7 %) postoperative periods (p < 0.01), decreased length of stay (5 vs. 7 days; p = 0.01), and increased likelihood of receiving adjuvant therapy (82 vs. 51 %; p < 0.01). There was no difference in the number of lymph nodes retrieved (median 20 in both groups), major morbidity, or 30-day mortality.
Conclusions: Laparoscopic gastrectomy for gastric adenocarcinoma is safe and effective for select patients in the West.
Figures
References
-
- Hayashi H, Ochiai T, Shimada H, Gunji Y. Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer. Surg Endosc. 2005;19:1172–6. - PubMed
-
- Kim HH, Hyung WJ, Cho GS, et al. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report—a phase III multicenter, prospective, randomized Trial (KLASS Trial) Ann Surg. 2010;251:417–20. - PubMed
-
- Kim YW, Baik YH, Yun YH, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008;248:721–7. - PubMed
-
- Lee JH, Han HS, Lee JH. A prospective randomized study comparing open vs laparoscopy-assisted distal gastrectomy in early gastric cancer: early results. Surg Endosc. 2005;19:168–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
