

Benign esophageal lesions: endoscopic and pathologic features
- PMID: 25632181
- PMCID: PMC4306152
- DOI: 10.3748/wjg.v21.i4.1091
Benign esophageal lesions: endoscopic and pathologic features
Abstract
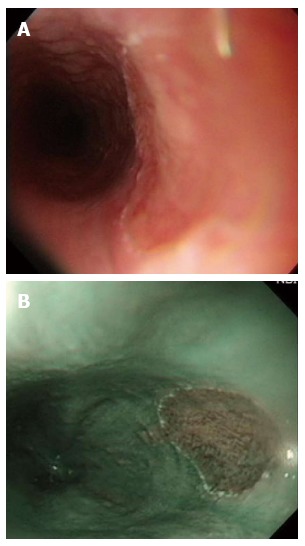
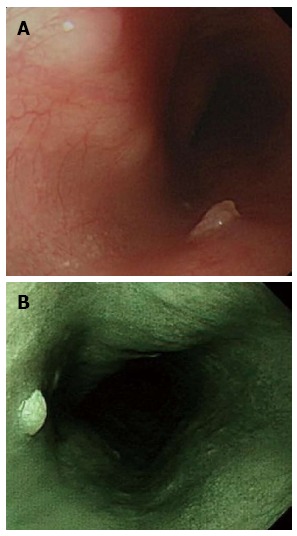
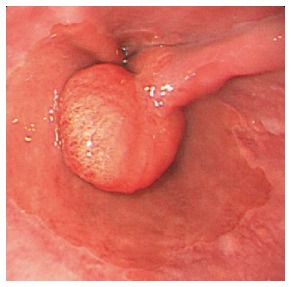
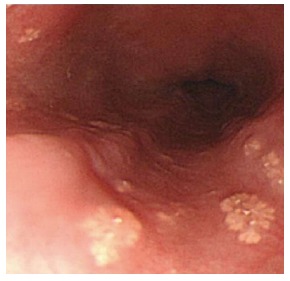
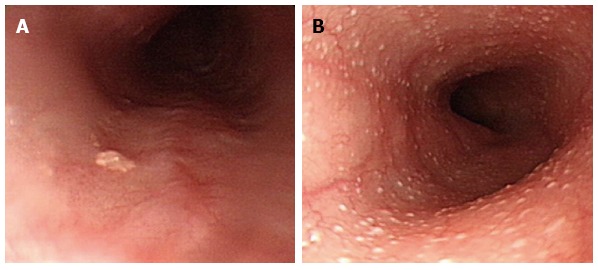
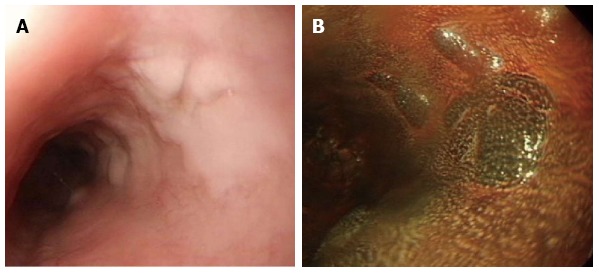
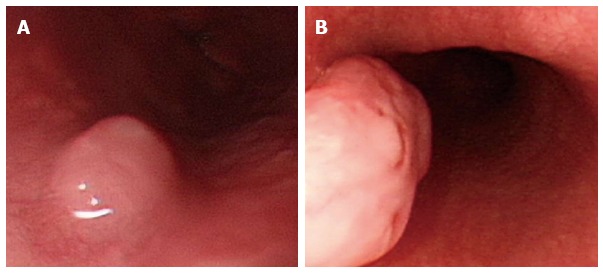
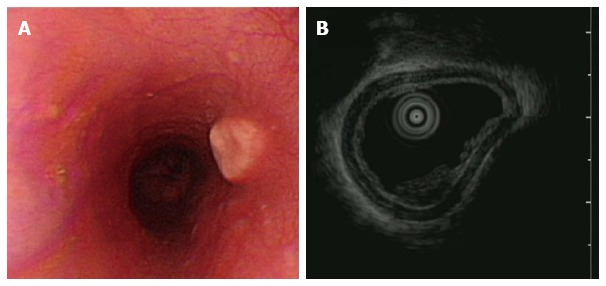
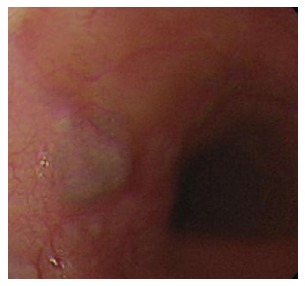
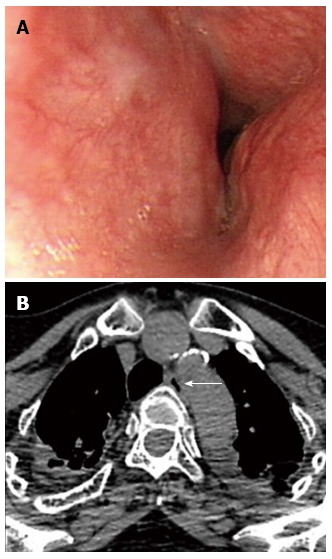
Benign esophageal lesions have a wide spectrum of clinical and pathologic features. Understanding the endoscopic and pathologic features of esophageal lesions is essential for their detection, differential diagnosis, and management. The purpose of this review is to provide updated features that may help physicians to appropriately manage these esophageal lesions. The endoscopic features of 2997 patients are reviewed. In epithelial lesions, the frequency of occurrence was in the following order: glycogenic acanthosis, heterotopic gastric mucosa, squamous papilloma, hyperplastic polyp, ectopic sebaceous gland and xanthoma. In subepithelial lesions, the order was as follows: hemangioma, leiomyoma, dysphagia aortica and granular cell tumor. Most benign esophageal lesions can be diagnosed according to their endoscopic appearance and findings on routine biopsy, and submucosal lesions, by endoscopic resection. Management is generally based upon the confidence of diagnosis and whether the lesion causes symptoms. We suggest endoscopic resection of all granular cell tumors and squamous papillomas because, while rare, these lesions have malignant potential. Dysphagia aortica should be considered in the differential diagnosis of dysphagia in the elderly.
Keywords: Benign tumor; Endoscopy; Epithelial lesions; Esophagus; Subepithelial lesions.
Figures
References
-
- Choong CK, Meyers BF. Benign esophageal tumors: introduction, incidence, classification, and clinical features. Semin Thorac Cardiovasc Surg. 2003;15:3–8. - PubMed
-
- Attah EB, Hajdu SI. Benign and malignant tumors of the esophagus at autopsy. J Thorac Cardiovasc Surg. 1968;55:396–404. - PubMed
-
- Lewis RB, Mehrotra AK, Rodriguez P, Levine MS. From the radiologic pathology archives: esophageal neoplasms: radiologic-pathologic correlation. Radiographics. 2013;33:1083–1108. - PubMed
-
- Yüksel I, Usküdar O, Köklü S, Başar O, Gültuna S, Unverdi S, Oztürk ZA, Sengül D, Arikök AT, Yüksel O, et al. Inlet patch: associations with endoscopic findings in the upper gastrointestinal system. Scand J Gastroenterol. 2008;43:910–914. - PubMed
-
- Maconi G, Pace F, Vago L, Carsana L, Bargiggia S, Bianchi Porro G. Prevalence and clinical features of heterotopic gastric mucosa in the upper oesophagus (inlet patch) Eur J Gastroenterol Hepatol. 2000;12:745–749. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
