

Reactive hemophagocytic syndrome in adult-onset Still disease: clinical features, predictive factors, and prognosis in 21 patients
- PMID: 25634183
- PMCID: PMC4602979
- DOI: 10.1097/MD.0000000000000451
Reactive hemophagocytic syndrome in adult-onset Still disease: clinical features, predictive factors, and prognosis in 21 patients
Abstract
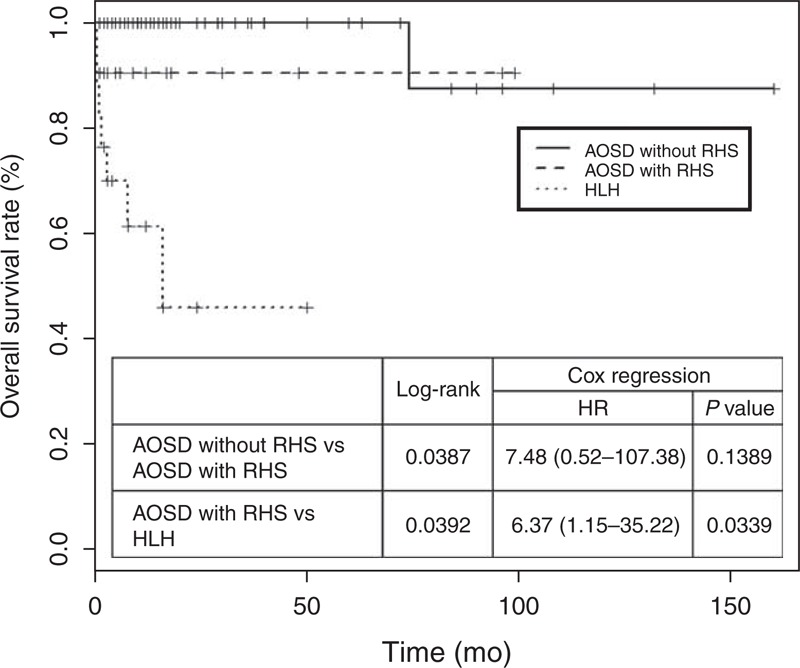
Hemophagocytic syndrome (HPS) is a potentially life-threatening complication of systemic inflammatory disorders. Adult-onset Still disease (AOSD) is one of the systemic autoimmune diseases associated with reactive hemophagocytic syndrome (RHS). This study aimed to evaluate the characteristic findings, predictive factors, and prognosis of RHS in patients with AOSD. We retrospectively evaluated 109 patients diagnosed with AOSD and reviewed their clinical data and laboratory findings, including the biopsy results of 21 AOSD patients with RHS. Moreover, data from 17 hemophagocytic lymphohistiocytosis (HLH) patients evaluated during the same period were compared with those from the RHS patients. Twenty-one patients (19.3%) developed RHS during the course of AOSD, and only 7 patients (6.4%) were confirmed by bone marrow, liver, or lymph node biopsy. AOSD patients with RHS showed significantly higher frequencies of splenomegaly, hepatomegaly, and lymphadenopathy than did those without RHS. Moreover, patients with RHS showed significantly higher relapse rates than those without RHS (61.9% vs 18.2%, P < 0.001). Possible triggering factors inducing hemophagocytosis were detected in 16 of 21 RHS patients (76.2%): disease flare in 12 patients (75%), infection in 3 patients (18.8%), and drug use in 1 patient (6.3%). AOSD patients with RHS showed higher frequencies of leukopenia, anemia, thrombocytopenia, hypoalbuminemia, hypofibrinogenemia, hypertriglyceridemia, hyperferritinemia, and elevated lactate dehydrogenase levels than did those without RHS. Multivariate logistic regression with forward selection procedure showed that low platelet count (<121,000/mm³), anemia, and hepatomegaly were independent predictors of RHS. Patients with definite RHS and those with probable RHS showed comparable results. Although RHS is a life-threatening complication of AOSD, long-term prognosis was observed to be similar in patients with and those without RHS. Compared to RHS patients, HLH patients had poor prognosis, such as higher death rates (52.9% vs 9.5%, P = 0.005). RHS can be considered when an AOSD patient shows at least 2 of the following 3 findings: low platelet count, anemia, and hepatomegaly. Diagnostic confirmation by biopsy may not be essential if typical clinical findings of RHS are present. Moreover, prognosis of RHS was better than that of HLH diagnosed by the presence of trilineage cytopenia at admission.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Ramos-Casals M, Brito-Zeron P, Lopez-Guillermo A, et al. Adult haemophagocytic syndrome. Lancet 2014; 383:1503–1516. - PubMed
-
- Janka GE. Hemophagocytic syndrome. Blood Rev 2007; 21:235–253. - PubMed
-
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol 2002; 14:548–552. - PubMed
-
- Larroche G, Mouthon L. Pathogenesis of hemopahgocytic syndrome. Autoimmun Rev 2004; 3:69–75. - PubMed
-
- Arceci RJ. Whem T cells and macrophage do not talk: the hemophagocytic syndrome. Curr Opin Hematol 2008; 15:359–367. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
