

A unique subset of epithelial ovarian cancers with platinum sensitivity and PARP inhibitor resistance
- PMID: 25634215
- PMCID: PMC4416405
- DOI: 10.1158/0008-5472.CAN-14-2593
A unique subset of epithelial ovarian cancers with platinum sensitivity and PARP inhibitor resistance
Abstract
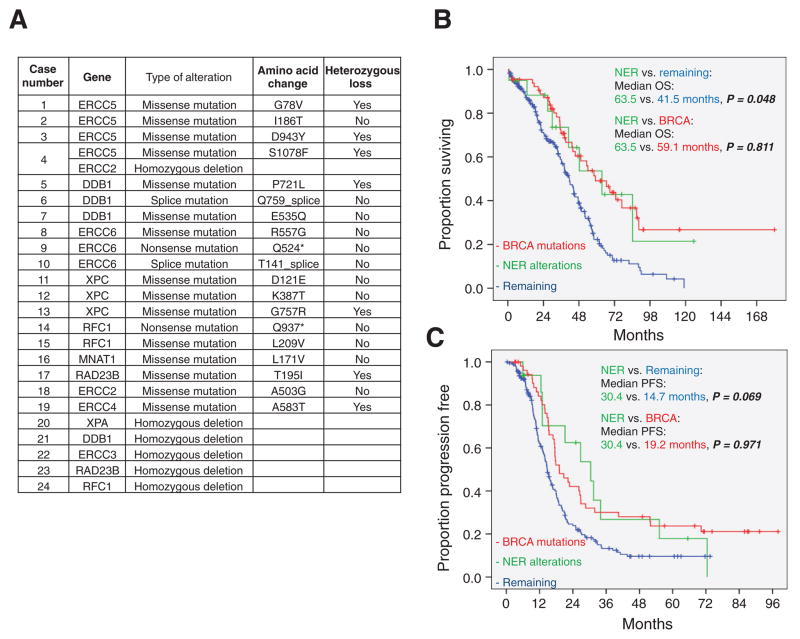
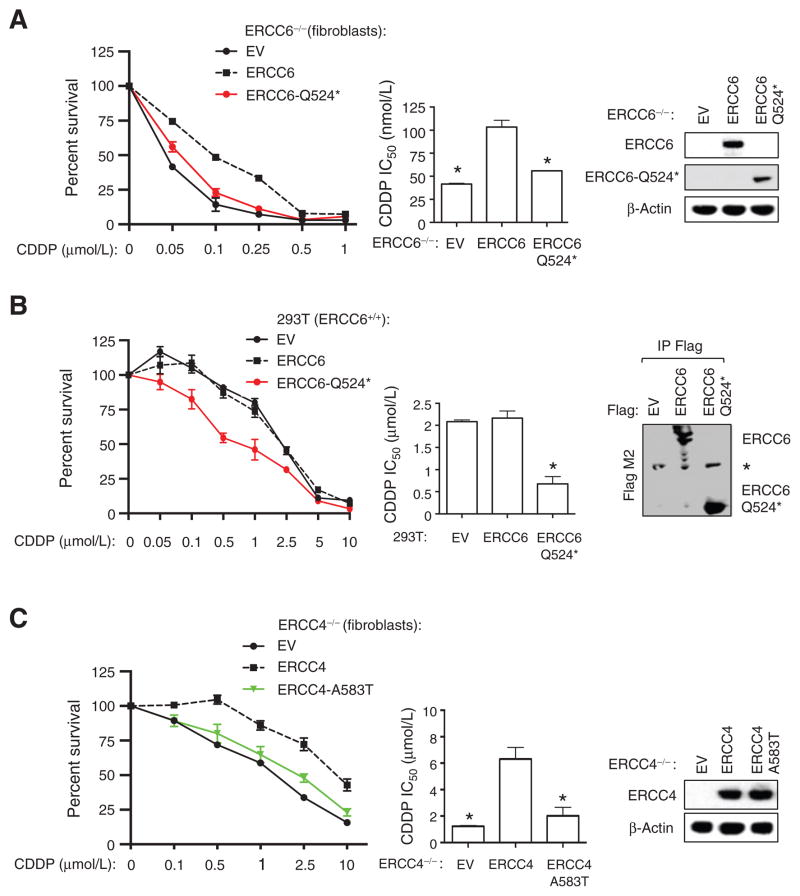
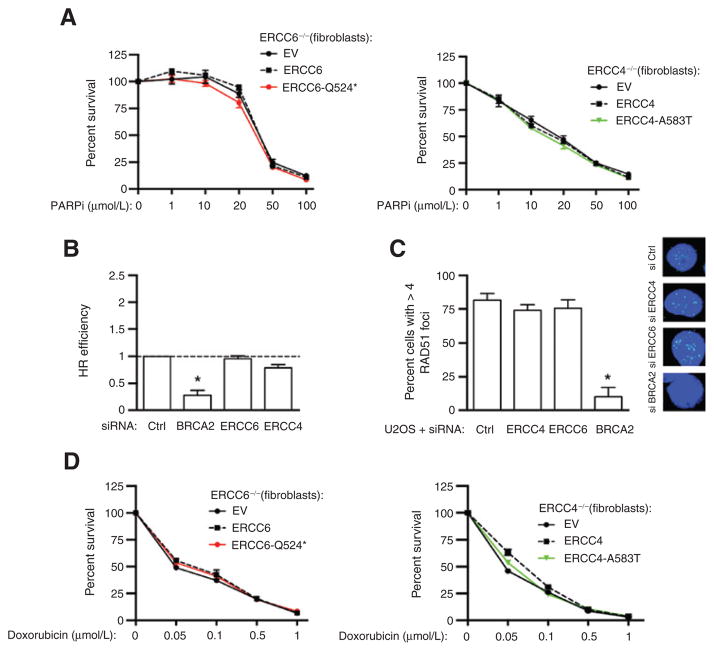
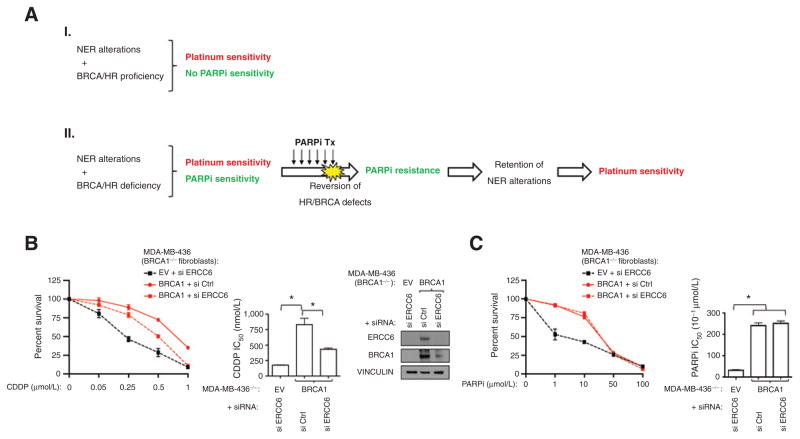
Platinum and PARP inhibitor (PARPi) sensitivity commonly coexist in epithelial ovarian cancer (EOC) due to the high prevalence of alterations in the homologous recombination (HR) DNA repair pathway that confer sensitivity to both drugs. In this report, we describe a unique subset of EOC with alterations in another DNA repair pathway, the nucleotide excision repair (NER) pathway, which may exhibit a discordance in sensitivities to these drugs. Specifically, 8% of high-grade serous EOC from The Cancer Genome Atlas dataset exhibited NER alterations, including nonsynonymous or splice site mutations and homozygous deletions of NER genes. Tumors with NER alterations were associated with improved overall survival (OS) and progression-free survival (PFS), compared with patients without NER alterations or BRCA1/2 mutations. Furthermore, patients with tumors with NER alterations had similar OS and PFS as BRCA1/2-mutated patients, suggesting that NER pathway inactivation in EOC conferred enhanced platinum sensitivity, similar to BRCA1/2-mutated tumors. Moreover, two NER mutations (ERCC6-Q524* and ERCC4-A583T), identified in the two most platinum-sensitive tumors, were functionally associated with platinum sensitivity in vitro. Importantly, neither NER alteration affected HR or conferred sensitivity to PARPi or other double-strand break-inducing agents. Overall, our findings reveal a new mechanism of platinum sensitivity in EOC that, unlike defective HR, may lead to a discordance in sensitivity to platinum and PARPi, with potential implications for previously reported and ongoing PARPi trials in this disease.
©2015 American Association for Cancer Research.
Conflict of interest statement
No potential confiicts of interest were disclosed.
Figures
Similar articles
-
Clinicopathological features of homologous recombination-deficient epithelial ovarian cancers: sensitivity to PARP inhibitors, platinum, and survival.Cancer Res. 2012 Nov 15;72(22):5675-82. doi: 10.1158/0008-5472.CAN-12-0324. Epub 2012 Oct 11. Cancer Res. 2012. PMID: 23066035 Clinical Trial.
-
ALDH1A1 Contributes to PARP Inhibitor Resistance via Enhancing DNA Repair in BRCA2-/- Ovarian Cancer Cells.Mol Cancer Ther. 2020 Jan;19(1):199-210. doi: 10.1158/1535-7163.MCT-19-0242. Epub 2019 Sep 18. Mol Cancer Ther. 2020. PMID: 31534014 Free PMC article.
-
Chemotherapy for Patients with BRCA1 and BRCA2-Mutated Ovarian Cancer: Same or Different?Am Soc Clin Oncol Educ Book. 2015:114-21. doi: 10.14694/EdBook_AM.2015.35.114. Am Soc Clin Oncol Educ Book. 2015. PMID: 25993149 Review.
-
Let-7e sensitizes epithelial ovarian cancer to cisplatin through repressing DNA double strand break repair.J Ovarian Res. 2017 Apr 4;10(1):24. doi: 10.1186/s13048-017-0321-8. J Ovarian Res. 2017. PMID: 28376831 Free PMC article.
-
Homologous recombination deficiency and ovarian cancer.Eur J Cancer. 2016 Jun;60:49-58. doi: 10.1016/j.ejca.2016.03.005. Epub 2016 Apr 9. Eur J Cancer. 2016. PMID: 27065456 Review.
Cited by
-
Translational and clinical implications of the genetic landscape of prostate cancer.Nat Rev Clin Oncol. 2016 Oct;13(10):597-610. doi: 10.1038/nrclinonc.2016.76. Epub 2016 Jun 1. Nat Rev Clin Oncol. 2016. PMID: 27245282 Free PMC article. Review.
-
Molecular mechanisms of cisplatin resistance in ovarian cancer.Genes Dis. 2023 Aug 2;11(6):101063. doi: 10.1016/j.gendis.2023.06.032. eCollection 2024 Nov. Genes Dis. 2023. PMID: 39224110 Free PMC article. Review.
-
NSD1 mutations by HPV status in head and neck cancer: differences in survival and response to DNA-damaging agents.Cancers Head Neck. 2019 Jul 8;4:3. doi: 10.1186/s41199-019-0042-3. eCollection 2019. Cancers Head Neck. 2019. PMID: 31321084 Free PMC article.
-
Toward More Comprehensive Homologous Recombination Deficiency Assays in Ovarian Cancer Part 2: Medical Perspectives.Cancers (Basel). 2022 Feb 21;14(4):1098. doi: 10.3390/cancers14041098. Cancers (Basel). 2022. PMID: 35205846 Free PMC article. Review.
-
Platinum Resistance After PARPi Resistance in a gBRCAmt Recurrent Ovarian Cancer Patient: a Case Report.Reprod Sci. 2023 Feb;30(2):615-621. doi: 10.1007/s43032-022-01037-3. Epub 2022 Aug 9. Reprod Sci. 2023. PMID: 35943701
References
-
- Konstantinopoulos PA, Awtrey CS. Management of ovarian cancer: a 75-year-old woman who has completed treatment. JAMA. 2012;307:1420–9. - PubMed
-
- Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, Lopez E, et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature. 2005;434:913–7. - PubMed
-
- Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005;434:917–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
