

Discrimination of Tumorous Intracerebral Hemorrhage from Benign Causes Using CT Densitometry
- PMID: 25634719
- PMCID: PMC7990598
- DOI: 10.3174/ajnr.A4233
Discrimination of Tumorous Intracerebral Hemorrhage from Benign Causes Using CT Densitometry
Abstract
Background and purpose: Differentiation of tumorous intracerebral hemorrhage from benign etiology is critical in initial treatment plan and prognosis. Our aim was to investigate the diagnostic value of CT densitometry to discriminate tumorous and nontumorous causes of acute intracerebral hemorrhage.
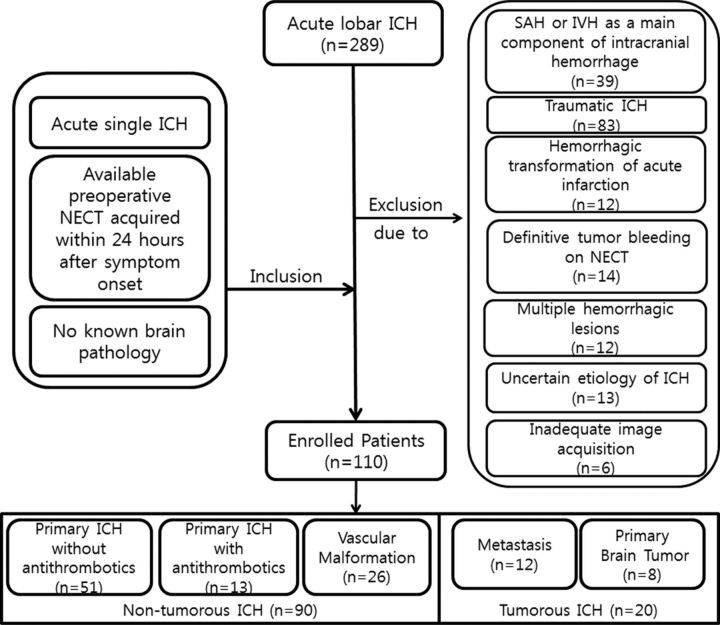
Materials and methods: This retrospective study included 110 patients with acute intracerebral hemorrhage classified into 5 groups: primary intracerebral hemorrhage without (group 1) or with antithrombotics (group 2) and secondary intracerebral hemorrhage with vascular malformation (group 3), brain metastases (group 4), or primary brain tumors (group 5). The 5 groups were dichotomized into tumorous (groups 4 and 5) and nontumorous intracerebral hemorrhage (groups 1-3). Histogram parameters of hematoma attenuation on nonenhanced CT were compared among the groups and between tumorous and nontumorous intracerebral hemorrhages. With receiver operating characteristic analysis, optimal cutoffs and area under the curve were calculated for discriminating tumorous and nontumorous intracerebral hemorrhages.
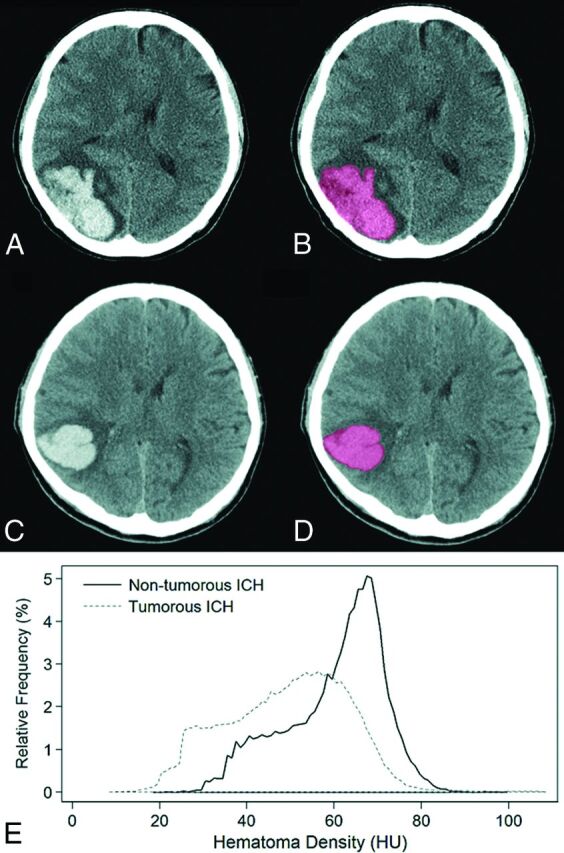
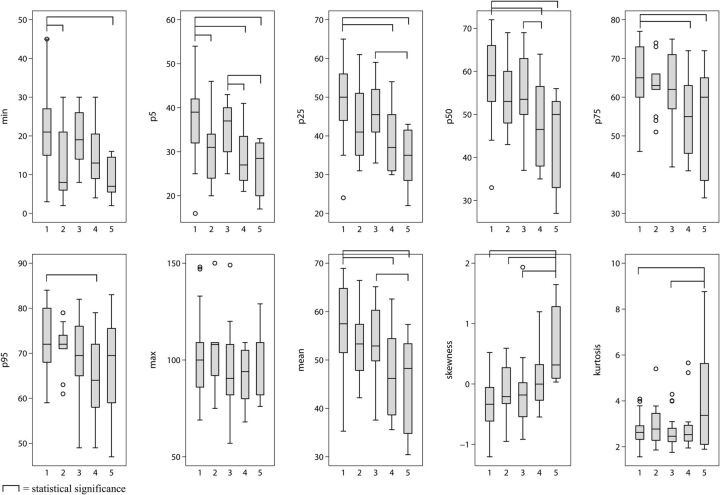
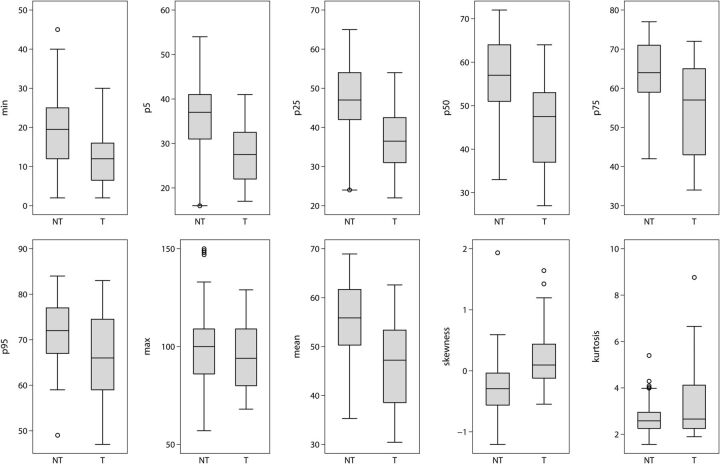
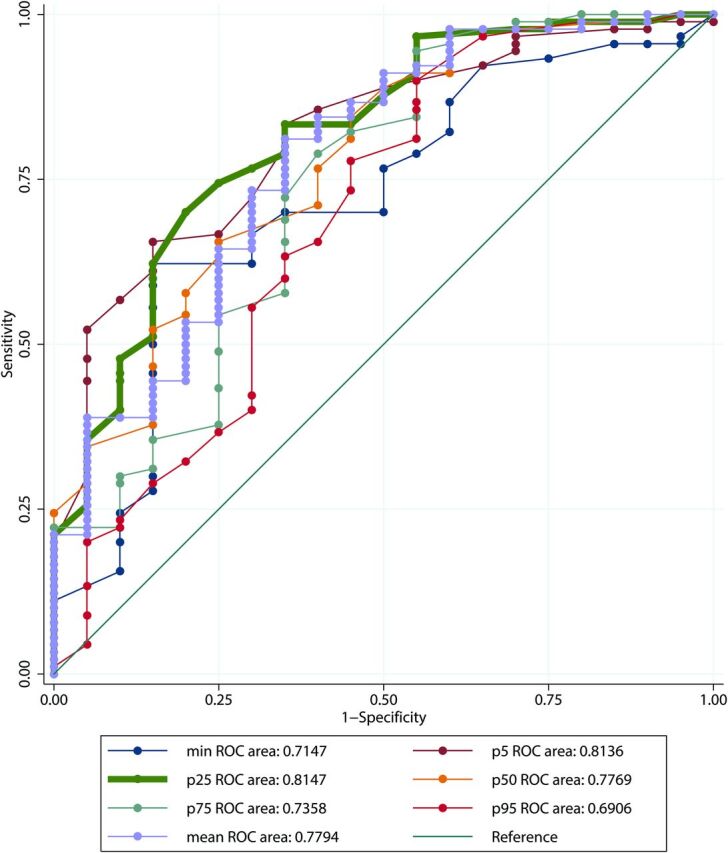
Results: Histogram analysis of acute intracerebral hemorrhage attenuation showed that group 1 had higher mean, 5th, 25th, 50th, and 75th percentile values than groups 4 and 5 and higher minimum and 5th percentile values than group 2. Group 3 had higher 5th percentile values than groups 4 and 5. After dichotomization, all histogram parameters except maximum and kurtosis were different between tumorous and nontumorous intracerebral hemorrhages, with tumors having lower cumulative histogram parameters and positive skewness. In receiver operating characteristic analysis, 5th and 25th percentile values showed the highest diagnostic performance for discriminating tumorous and nontumorous intracerebral hemorrhages, with 0.81 area under the curve, cutoffs of 34 HU and 44 HU, sensitivities of 65.6% and 70.0%, and specificities of 85.0% and 80.0%, respectively.
Conclusions: CT densitometry of intracerebral hemorrhage on nonenhanced CT might be useful for discriminating tumorous and nontumorous causes of acute intracerebral hemorrhage.
© 2015 by American Journal of Neuroradiology.
Figures
Similar articles
-
Neoplastic and Non-Neoplastic Causes of Acute Intracerebral Hemorrhage on CT : The Diagnostic Value of Perihematomal Edema.Clin Neuroradiol. 2020 Jun;30(2):271-278. doi: 10.1007/s00062-019-00774-4. Epub 2019 Mar 21. Clin Neuroradiol. 2020. PMID: 30899965
-
Dual-energy CT in the evaluation of intracerebral hemorrhage of unknown origin: differentiation between tumor bleeding and pure hemorrhage.AJNR Am J Neuroradiol. 2012 May;33(5):865-72. doi: 10.3174/ajnr.A2890. Epub 2012 Jan 12. AJNR Am J Neuroradiol. 2012. PMID: 22241388 Free PMC article.
-
CT histogram analysis to distinguish between acute intracerebral hemorrhage and cavernous hemangioma.Clin Radiol. 2024 Nov;79(11):872-879. doi: 10.1016/j.crad.2024.07.013. Epub 2024 Jul 20. Clin Radiol. 2024. PMID: 39129104
-
[Spontaneous intracerebral hemorrhage: the clinical neuroradiological view].Radiologe. 1999 Oct;39(10):828-37. doi: 10.1007/s001170050719. Radiologe. 1999. PMID: 10550381 Review. German.
-
Etiologies of intracerebral hematomas.Curr Atheroscler Rep. 2012 Aug;14(4):314-21. doi: 10.1007/s11883-012-0253-0. Curr Atheroscler Rep. 2012. PMID: 22562528 Review.
Cited by
-
A Radiomics Nomogram for Classifying Hematoma Entities in Acute Spontaneous Intracerebral Hemorrhage on Non-contrast-Enhanced Computed Tomography.Front Neurosci. 2022 Jun 10;16:837041. doi: 10.3389/fnins.2022.837041. eCollection 2022. Front Neurosci. 2022. PMID: 35757547 Free PMC article.
-
Editorial: Hemostasis and Stroke.Front Neurol. 2021 Aug 11;12:737556. doi: 10.3389/fneur.2021.737556. eCollection 2021. Front Neurol. 2021. PMID: 34456855 Free PMC article. No abstract available.
-
Air Pollution and Intracranial Hemorrhage.Ann Indian Acad Neurol. 2022 Sep;25(Suppl 1):S22-S25. doi: 10.4103/aian.aian_1131_21. Epub 2022 Mar 25. Ann Indian Acad Neurol. 2022. PMID: 36213099 Free PMC article.
-
An Explainable AI Exploration of the Machine Learning Classification of Neoplastic Intracerebral Hemorrhage from Non-Contrast CT.Cancers (Basel). 2025 Jul 29;17(15):2502. doi: 10.3390/cancers17152502. Cancers (Basel). 2025. PMID: 40805199 Free PMC article.
-
Building nonenhanced CT based radiomics model in discriminating arteriovenous malformation related hematomas from hypertensive intracerebral hematomas.Front Neurosci. 2023 Nov 28;17:1284560. doi: 10.3389/fnins.2023.1284560. eCollection 2023. Front Neurosci. 2023. PMID: 38089971 Free PMC article.
References
-
- Qureshi AI, Tuhrim S, Broderick JP, et al. . Spontaneous intracerebral hemorrhage. N Engl J Med 2001;344:1450–60 - PubMed
-
- Broderick JP, Brott T, Tomsick T, et al. . The risk of subarachnoid and intracerebral hemorrhages in blacks as compared with whites. N Engl J Med 1992;326:733–36 - PubMed
-
- Furlan AJ, Whisnant JP, Elveback LR. The decreasing incidence of primary intracerebral hemorrhage: a population study. Ann Neurol 1979;5:367–73 - PubMed
-
- Sacco S, Marini C, Toni D, et al. . Incidence and 10-year survival of intracerebral hemorrhage in a population-based registry. Stroke 2009;40:394–99 - PubMed
-
- Foulkes MA, Wolf PA, Price TR, et al. . The Stroke Data Bank: design, methods, and baseline characteristics. Stroke 1988;19:547–54 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical