

Progression of pediatric CKD of nonglomerular origin in the CKiD cohort
- PMID: 25635034
- PMCID: PMC4386256
- DOI: 10.2215/CJN.07480714
Progression of pediatric CKD of nonglomerular origin in the CKiD cohort
Abstract
Background and objectives: Congenital anomalies of the kidney and urinary tract and genetic disorders cause most cases of CKD in children. This study evaluated the relationships between baseline proteinuria and BP and longitudinal changes in GFR in children with these nonglomerular causes of CKD.
Design, setting, participants, & measurements: Urine protein-to-creatinine ratio, casual systolic and diastolic BP (normalized for age, sex, and height), and GFR decline were assessed in the prospective CKD in Children cohort study.
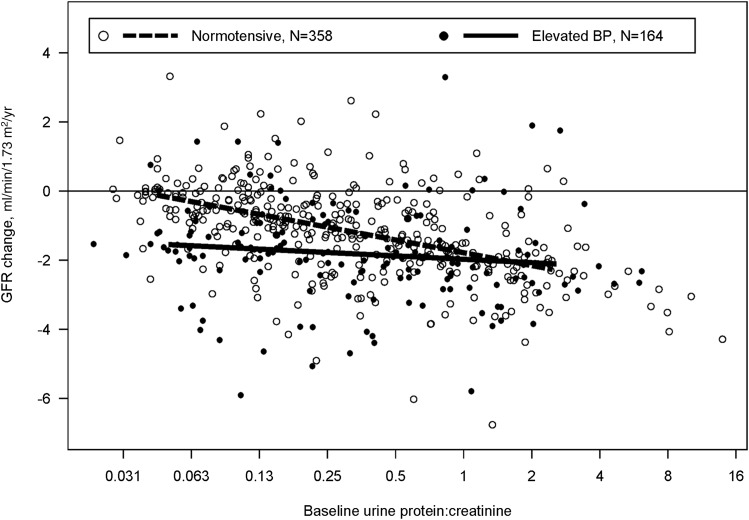
Results: A total of 522 children, median age 10 years (interquartile range, 7, 14 years) with nonglomerular CKD were followed for a median of 4.4 years. The mean baseline GFR in the cohort was 52 ml/min per 1.73 m(2) (95% confidence interval [95% CI], 50 to 54) and declined 1.3 ml/min per 1.73 m(2) per year on average (95%CI, 1.6 to 1.1). A 2-fold higher baseline urine protein-to-creatinine ratio was associated with an accelerated GFR decline of 0.3 ml/min per 1.73 m(2) per year (95% CI, 0.4 to 0.1). A 1-unit higher baseline systolic BP z-score was associated with an additional GFR decline of 0.4 ml/min per 1.73 m(2) per year (95% CI, 0.7 to 0.1). Among normotensive children, larger GFR declines were associated with larger baseline urine protein-to-creatinine ratios; eGFR declines of 0.8 and 1.8 ml/min per 1.73 m(2) per year were associated with urine protein-to-creatinine ratio <0.5 and ≥0.5 mg/mg, respectively. Among children with elevated BP, average GFR declines were evident but were not larger in children with higher levels of proteinuria.
Conclusions: Baseline proteinuria and systolic BP levels are independently associated with CKD progression in children with nonglomerular CKD.
Keywords: chronic kidney disease; hypertension; proteinuria; renal progression.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Schaefer B, Wühl E: Educational paper: Progression in chronic kidney disease and prevention strategies. Eur J Pediatr 171: 1579–1588, 2012 - PubMed
-
- Ishikura K, Uemura O, Hamasaki Y, Ito S, Wada N, Hattori M, Ohashi Y, Tanaka R, Nakanishi K, Kaneko T, Honda M, Pediatric CKD Study Group in Japan. Committee of Measures for Pediatric CKD of Japanese Society of Pediatric Nephrology : Progression to end-stage kidney disease in Japanese children with chronic kidney disease: results of a nationwide prospective cohort study. Nephrol Dial Transplant 29: 878–884, 2014 - PubMed
-
- Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, Marcantoni C, de Jong PE, de Zeeuw D, Shahinfar S, Ruggenenti P, Remuzzi G, Levey AS, AIPRD Study Group. Angiotensin-Converting Enzymne Inhibition and Progression of Renal Disease : Proteinuria as a modifiable risk factor for the progression of non-diabetic renal disease. Kidney Int 60: 1131–1140, 2001 - PubMed
-
- Taal MW, Brenner BM: Defining renal risk. Curr Opin Nephrol Hypertens 16: 554–556, 2007 - PubMed
-
- Wühl E, Mehls O, Schaefer F, ESCAPE Trial Group : Antihypertensive and antiproteinuric efficacy of ramipril in children with chronic renal failure. Kidney Int 66: 768–776, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
