

Emergency department diagnosis of pulmonary hypertension in a patient with left atrial sarcoma
- PMID: 25635192
- PMCID: PMC4306056
- DOI: 10.1186/s12245-014-0032-5
Emergency department diagnosis of pulmonary hypertension in a patient with left atrial sarcoma
Abstract
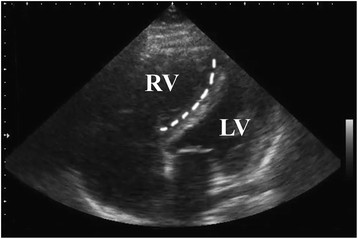
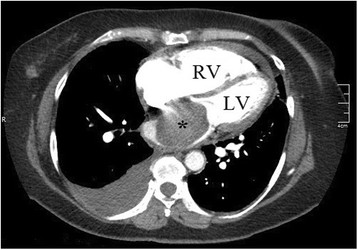
Pulmonary hypertension is a disease with many etiologies and is responsible for 200,000 admissions and 25,000 hospitalizations in the United States each year. We report the case of a previously healthy 58-year-old woman who presented to the emergency department with a months-long history of worsening dyspnea on exertion, orthopnea, and paroxysmal nocturnal dyspnea. Despite the severity of her symptoms, she had no corroborative physical exam findings, including jugular venous distension or peripheral edema. Bedside emergency department ultrasonography revealed a dilated right ventricle and bowing of the intraventricular septum into the left ventricle, consistent with pulmonary hypertension. CT angiography of the chest performed in the emergency department revealed a large left atrial mass, found on pathology to be a left atrial sarcoma. This case illustrates how severely symptomatic pulmonary hypertension can have few to no physical exam findings and the utility of bedside emergency department ultrasound in making the presumptive diagnosis.
Figures
Similar articles
-
Novel technique of repairing right partial anomalous pulmonary venous connection with intact atrial septum using in situ interatrial septum as a flap in a 68-year-old-woman: a case report.J Cardiothorac Surg. 2020 Sep 25;15(1):269. doi: 10.1186/s13019-020-01313-w. J Cardiothorac Surg. 2020. PMID: 32977845 Free PMC article.
-
Bevacizumab: A Rare Cause of Nonischemic Cardiomyopathy.Case Rep Cardiol. 2018 Aug 27;2018:1361326. doi: 10.1155/2018/1361326. eCollection 2018. Case Rep Cardiol. 2018. PMID: 30225147 Free PMC article.
-
Atrial septal defect in an elderly woman-a case report.J Med Life. 2011 Jan-Mar;4(1):91-3. Epub 2011 Feb 25. J Med Life. 2011. PMID: 21505579 Free PMC article.
-
Paraneoplastic Encephalopathy in a Patient With Metastatic Lung Cancer: A Case Study.J Adv Pract Oncol. 2018 Mar;9(2):216-221. Epub 2018 Mar 1. J Adv Pract Oncol. 2018. PMID: 30588355 Free PMC article. Review.
-
Does this dyspneic patient in the emergency department have congestive heart failure?JAMA. 2005 Oct 19;294(15):1944-56. doi: 10.1001/jama.294.15.1944. JAMA. 2005. PMID: 16234501 Review.
Cited by
-
Demographics and Outcomes of Pulmonary Hypertension Patients in United States Emergency Departments.West J Emerg Med. 2020 Apr 16;21(3):714-721. doi: 10.5811/westjem.2020.2.45187. West J Emerg Med. 2020. PMID: 32421524 Free PMC article.
References
-
- Rich S. In: Harrison's Principles of Internal Medicine. 18. Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J, editor. McGraw-Hill, New York; 2011. Pulmonary hypertension; pp. 1576–1581.
-
- Braithwaite S, Perina D. In: Rosen's Emergency Medicine. 8. Marx J, Hockberger R, Walls R, editor. Saunders, Philadelphia; 2014. Dyspnea; pp. 206–213.
LinkOut - more resources
Full Text Sources
Other Literature Sources
