

Does MOG Ig-positive AQP4-seronegative opticospinal inflammatory disease justify a diagnosis of NMO spectrum disorder?
- PMID: 25635259
- PMCID: PMC4309526
- DOI: 10.1212/NXI.0000000000000062
Does MOG Ig-positive AQP4-seronegative opticospinal inflammatory disease justify a diagnosis of NMO spectrum disorder?
Abstract
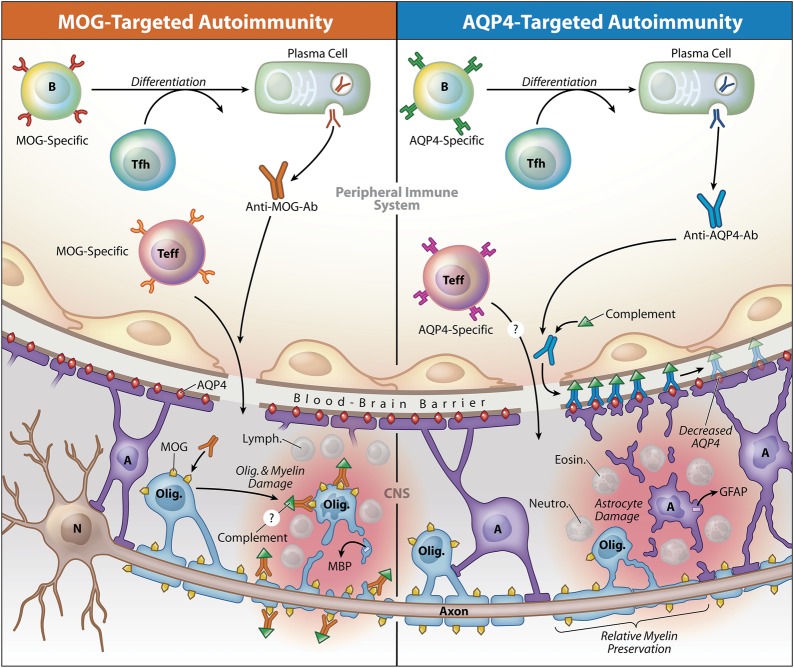
While neuromyelitis optica (NMO) immunoglobulin (Ig) G is considered the hallmark serologic marker of NMO, its association is not absolute, as NMO IgG is not detected in approximately one-fourth of the patients diagnosed with NMO spectrum disorder (NMOSD). Thus, the recent discovery that antibodies to myelin oligodendrocyte glycoprotein (MOG) are detected in some NMO IgG-seronegative patients manifesting clinical and neuroimaging signs of NMO or NMOSD has created tremendous excitement. However, it may be premature to classify this subgroup as NMOSD. NMO is considered an autoimmune astrocytopathy, and aquaporin-4 (AQP4), expressed on astrocytes, is recognized as the target autoantigen of NMO IgG. As its name denotes, MOG is produced by oligodendrocytes, CNS myelin-producing cells, and MOG is well-recognized as one of the candidate autoantigens in multiple sclerosis (MS) and acute disseminated encephalomyelitis (ADEM). Thus, is it possible that the clinical NMOSD-like phenotype associated with MOG-specific antibodies represents a variant of opticospinal MS or ADEM but not AQP4 autoimmunity or NMOSD? Whether this MOG-Ig positive AQP4-seronegative phenotype should be classified as NMOSD, opticospinal MS, or a unique entity is not simply a theoretical question but rather has practical implications for patients, their physicians, insurance carriers, and clinical investigators conducting NMO treatment trials.
Figures
References
-
- Jarius S, Wildemann B. AQP4 antibodies in neuromyelitis optica: diagnostic and pathogenetic relevance. Nat Rev Neurol 2010;6:383–392. - PubMed
-
- Pittock SJ, Lennon VA, de Seze J, et al. Neuromyelitis optica and non organ-specific autoimmunity. Arch Neurol 2008;65:78–83. - PubMed
-
- Kitley J, Waters P, Woodhall M, et al. Neuromyelitis optica spectrum disorders with aquaporin-4 and myelin-oligodendrocyte glycoprotein antibodies: a comparative study. JAMA Neurol 2014;71:276–283. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials