

Hypertonic saline for brain relaxation and intracranial pressure in patients undergoing neurosurgical procedures: a meta-analysis of randomized controlled trials
- PMID: 25635862
- PMCID: PMC4311961
- DOI: 10.1371/journal.pone.0117314
Hypertonic saline for brain relaxation and intracranial pressure in patients undergoing neurosurgical procedures: a meta-analysis of randomized controlled trials
Abstract
Background: A wealth of evidence from randomized controlled trials (RCTs) has indicated that hypertonic saline (HS) is at least as effective as, if not better than, mannitol in the treatment of increased intracranial pressure(ICP). However, there is little known about the effects of HS in patients during neurosurgery. Thus, this meta-analysis was performed to compare the intraoperative effects of HS with mannitol in patients undergoing craniotomy.
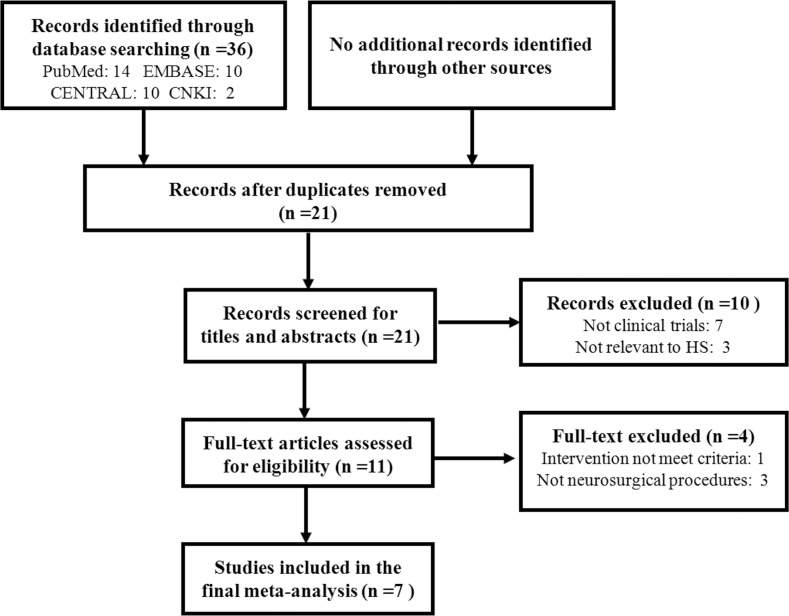
Methods: According to the research strategy, we searched PUBMED, EMBASE and Cochrane Central Register of Controlled Trials. Other sources such as the internet-based clinical trial registries and conference proceedings were also searched. After literature searching, two investigators independently performed literature screening, quality assessment of the included trials and data extraction. The outcomes included intraoperative brain relaxation, intraoperative ICP, total volume of fluid required, diuresis, hemodynamic parameters, electrolyte level, mortality or dependence and adverse events.
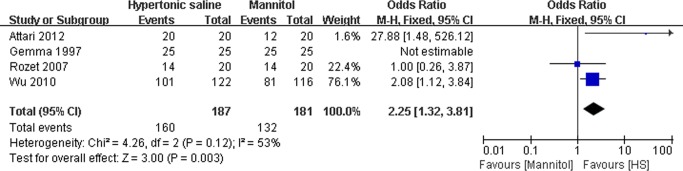
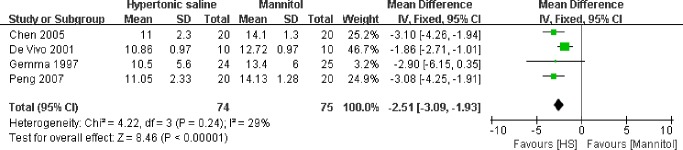
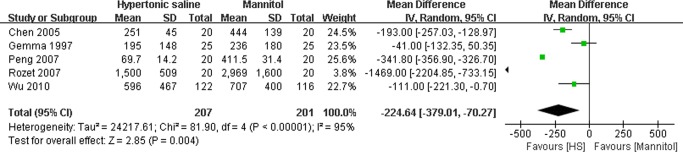
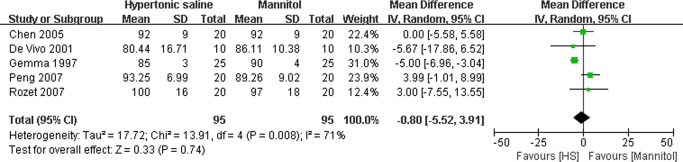
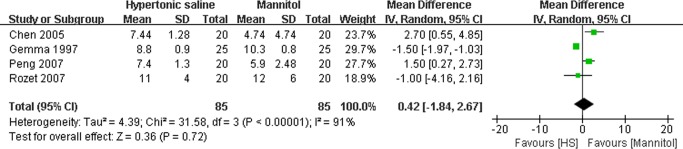
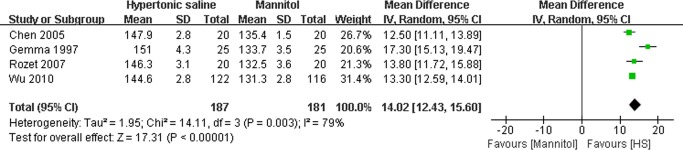
Results: Seven RCTs with 468 participants were included. The quality of the included trials was acceptable. HS could significantly increase the odds of satisfactory intraoperative brain relaxation (OR: 2.25, 95% CI: 1.32-3.81; P = 0.003) and decrease the mean difference (MD) of maximal ICP (MD: -2.51 mmHg, 95% CI: -3.39--1.93 mmHg; P<0.00001) in comparison with mannitol with no significant heterogeneity among the study results. Compared with HS, mannitol had a more prominent diuretic effect. And patients treated with HS had significantly higher serum sodium than mannitol-treated patients.
Conclusions: Considering that robust outcome measures are absent because brain relaxation and ICP can be influenced by several factors except for the hyperosmotic agents, the results of present meta-analysis should be interpreted with cautions. Well-designed RCTs in the future are needed to further test the present results, identify the impact of HS on the clinically relevant outcomes and explore the potential mechanisms of HS.
Conflict of interest statement
Figures


References
-
- Turner CR, Losasso TJ, Muzzi DA, Weglinski MR (1996) Brain relaxation and cerebrospinal fluid pressure during craniotomy for resection of supratentorial mass lesions. J Neurosurg Anesthesiol 8: 126–132. - PubMed
-
- Petersen KD, Landsfeldt U, Cold GE, Petersen CB, Mau S, et al. (2003) Intracranial pressure and cerebral hemodynamic in patients with cerebral tumors: a randomized prospective study of patients subjected to craniotomy in propofol-fentanyl, isoflurane-fentanyl, or sevoflurane-fentanyl anesthesia. Anesthesiology 98: 329–336. - PubMed
-
- Dinsmore J (2007) Anaesthesia for elective neurosurgery. Br J Anaesth 99: 68–74. - PubMed
-
- Infanti JL (2008) Challenging the gold standard: should mannitol remain our first-line defense against intracranial hypertension? J Neurosci Nurs 40: 362–368. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
