

Bleeding and infection with external ventricular drainage: a systematic review in comparison with adjudicated adverse events in the ongoing Clot Lysis Evaluating Accelerated Resolution of Intraventricular Hemorrhage Phase III (CLEAR-III IHV) trial
- PMID: 25635887
- PMCID: PMC4333009
- DOI: 10.1227/NEU.0000000000000624
Bleeding and infection with external ventricular drainage: a systematic review in comparison with adjudicated adverse events in the ongoing Clot Lysis Evaluating Accelerated Resolution of Intraventricular Hemorrhage Phase III (CLEAR-III IHV) trial
Abstract
Background: Retrospective series report varied rates of bleeding and infection with external ventricular drainage (EVD). There have been no prospective studies of these risks with systematic surveillance, threshold definitions, or independent adjudication.
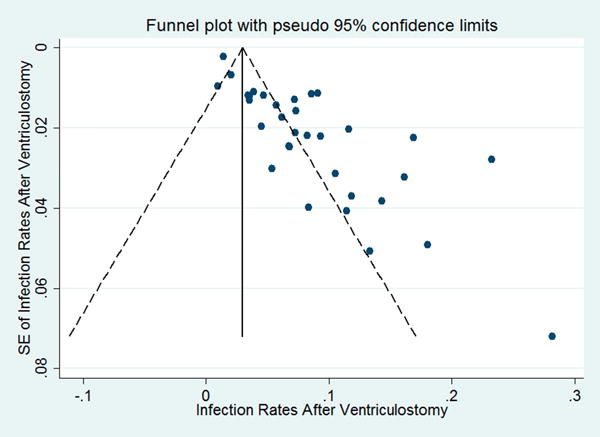
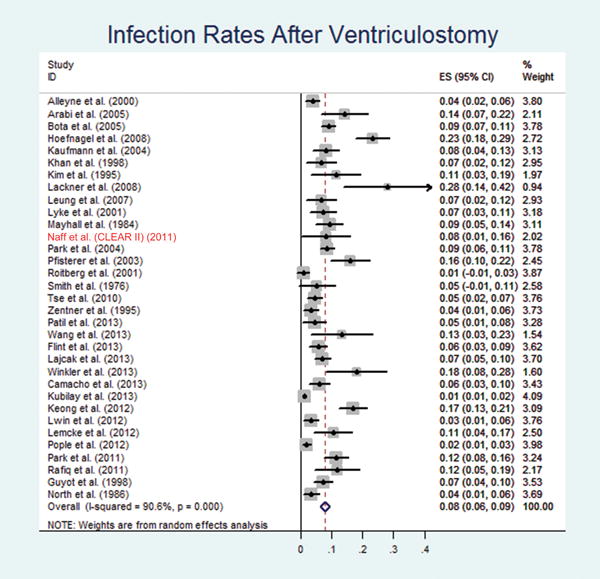
Objective: To analyze the rate of complications in the ongoing Clot Lysis: Evaluating Accelerated Resolution of Intraventricular Hemorrhage Phase III (CLEAR III) trial, providing a comparison with a systematic review of complications of EVD in the literature.
Methods: Patients were prospectively enrolled in the CLEAR III trial after placement of an EVD for obstructive intraventricular hemorrhage and randomized to receive recombinant tissue-type plasminogen activator or placebo. We counted any detected new hemorrhage (catheter tract hemorrhage or any other distant hemorrhage) on computed tomography scan within 30 days from the randomization. Meta-analysis of published series of EVD placement was compiled with STATA software.
Results: Growing or unstable hemorrhage was reported as a cause of exclusion from the trial in 74 of 5707 cases (1.3%) screened for CLEAR III. The first 250 patients enrolled have completed adjudication of adverse events. Forty-two subjects (16.8%) experienced ≥1 new bleeds or expansions, and 6 of 250 subjects (2.4%) suffered symptomatic hemorrhages. Eleven cases (4.4%) had culture-proven bacterial meningitis or ventriculitis.
Conclusion: Risks of bleeding and infection in the ongoing CLEAR III trial are comparable to those previously reported in EVD case series. In the present study, rates of new bleeds and bacterial meningitis/ventriculitis are very low despite multiple daily injections, blood in the ventricles, the use of thrombolysis in half the cases, and generalization to >60 trial sites.
Conflict of interest statement
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.
Figures




Similar articles
-
A multicenter, randomized, double-blinded, placebo-controlled phase III study of Clot Lysis Evaluation of Accelerated Resolution of Intraventricular Hemorrhage (CLEAR III).Int J Stroke. 2014 Jun;9(4):536-42. doi: 10.1111/ijs.12097. Epub 2013 Aug 28. Int J Stroke. 2014. PMID: 24033910 Free PMC article. Clinical Trial.
-
Symptomatic Hemorrhagic Complications in Clot Lysis: Evaluation of Accelerated Resolution of Intraventricular Hemorrhage Phase III Clinical Trial (CLEAR III): A Posthoc Root-Cause Analysis.Neurosurgery. 2018 Dec 1;83(6):1260-1268. doi: 10.1093/neuros/nyx587. Neurosurgery. 2018. PMID: 29294116 Free PMC article.
-
Permanent CSF shunting after intraventricular hemorrhage in the CLEAR III trial.Neurology. 2017 Jul 25;89(4):355-362. doi: 10.1212/WNL.0000000000004155. Epub 2017 Jun 28. Neurology. 2017. PMID: 28659429 Free PMC article. Clinical Trial.
-
Intraventricular fibrinolysis versus external ventricular drainage alone in intraventricular hemorrhage: a meta-analysis.Stroke. 2011 Oct;42(10):2776-81. doi: 10.1161/STROKEAHA.111.615724. Epub 2011 Aug 4. Stroke. 2011. PMID: 21817146
-
Fibrinolytics and Intraventricular Hemorrhage: A Systematic Review and Meta-analysis.Neurocrit Care. 2020 Feb;32(1):262-271. doi: 10.1007/s12028-019-00786-5. Neurocrit Care. 2020. PMID: 31376141 Free PMC article.
Cited by
-
Randomized, Open-Label, Phase 1/2a Study to Determine the Maximum Tolerated Dose of Intraventricular Sustained Release Nimodipine for Subarachnoid Hemorrhage (NEWTON [Nimodipine Microparticles to Enhance Recovery While Reducing Toxicity After Subarachnoid Hemorrhage]).Stroke. 2017 Jan;48(1):145-151. doi: 10.1161/STROKEAHA.116.014250. Epub 2016 Dec 8. Stroke. 2017. PMID: 27932607 Free PMC article. Clinical Trial.
-
Endoscope-assisted microsurgical evacuation versus external ventricular drainage for the treatment of cast intraventricular hemorrhage: results of a comparative series.Neurosurg Rev. 2020 Apr;43(2):695-708. doi: 10.1007/s10143-019-01110-7. Epub 2019 May 8. Neurosurg Rev. 2020. PMID: 31069562
-
The Insertion and Management of External Ventricular Drains: An Evidence-Based Consensus Statement : A Statement for Healthcare Professionals from the Neurocritical Care Society.Neurocrit Care. 2016 Feb;24(1):61-81. doi: 10.1007/s12028-015-0224-8. Neurocrit Care. 2016. PMID: 26738503 Review.
-
Use of flexible endoscopic aspiration for an intraventricular small floating clot with hemorrhage: a technical note.Neurosurg Rev. 2021 Aug;44(4):2363-2367. doi: 10.1007/s10143-020-01392-2. Epub 2020 Sep 19. Neurosurg Rev. 2021. PMID: 32951062
-
Incidence, Predictors, and Outcomes of Ventriculostomy-Associated Infections in Spontaneous Intracerebral Hemorrhage.Neurocrit Care. 2016 Jun;24(3):389-96. doi: 10.1007/s12028-015-0199-5. Neurocrit Care. 2016. PMID: 26337068
References
-
- Staykov D, Bardutzky J, Huttner HB, Schwab S. Intraventricular fibrinolysis for intracerebral hemorrhage with severe ventricular involvement. Neurocrit Care. 2011 Aug;15(1):194–209. - PubMed
-
- Engelhard HH, Andrews CO, Slavin KV, Charbel FT. Current management of intraventricular hemorrhage. Surg Neurol. 2003 Jul;60(1):15–21. discussion 21–12. - PubMed
-
- Nieuwkamp DJ, de Gans K, Rinkel GJ, Algra A. Treatment and outcome of severe intraventricular extension in patients with subarachnoid or intracerebral hemorrhage: a systematic review of the literature. J Neurol. 2000 Feb;247(2):117–121. - PubMed
-
- Nyquist P, LeDroux S, Geocadin R. Thrombolytics in intraventricular hemorrhage. Curr Neurol Neurosci Rep. 2007 Nov;7(6):522–528. - PubMed
-
- Naff NJ. Intraventricular Hemorrhage in Adults. Curr Treat Options Neurol. 1999 Jul;1(3):173–178. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
