

Interstitial Fibrosis Restricts Osmotic Water Transport in Encapsulating Peritoneal Sclerosis
- PMID: 25636412
- PMCID: PMC4587704
- DOI: 10.1681/ASN.2014090939
Interstitial Fibrosis Restricts Osmotic Water Transport in Encapsulating Peritoneal Sclerosis
Abstract
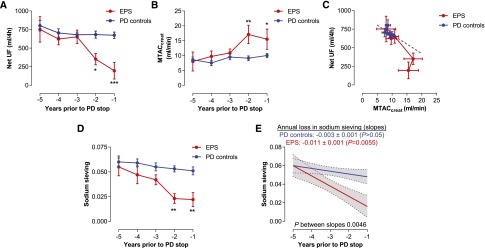
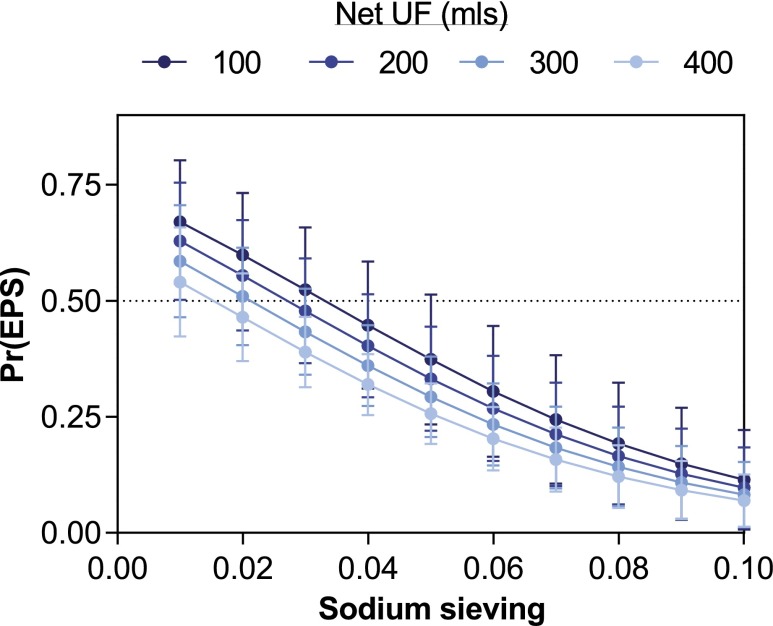
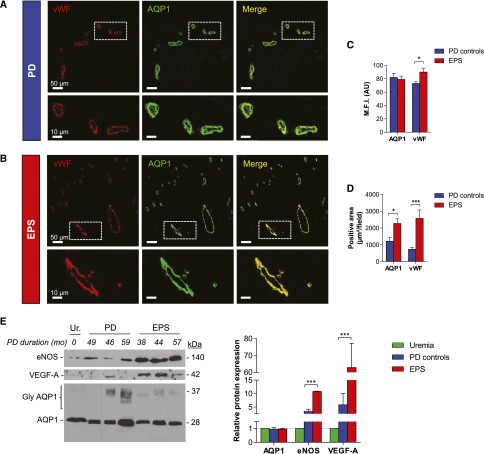
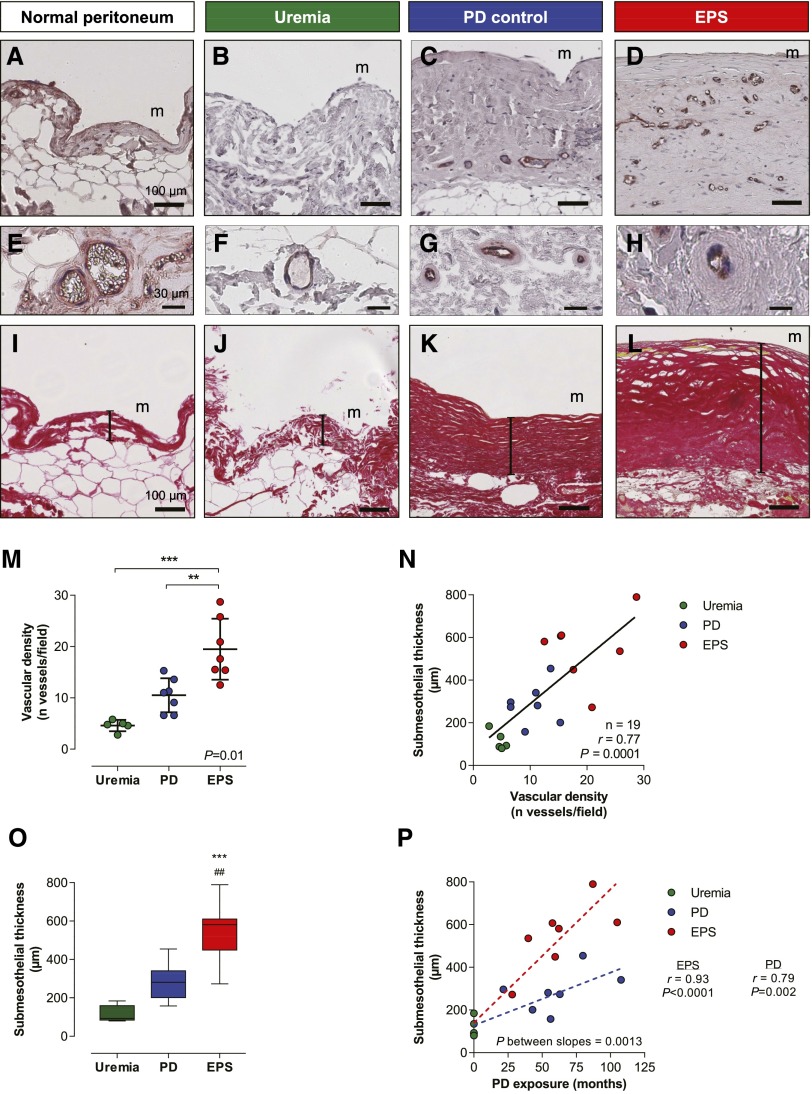
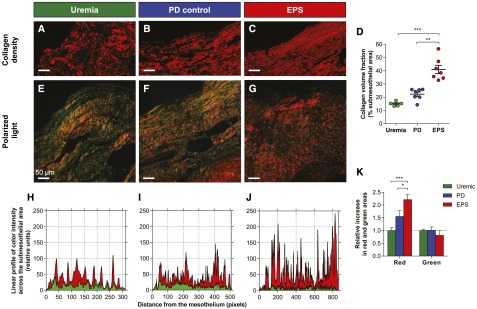
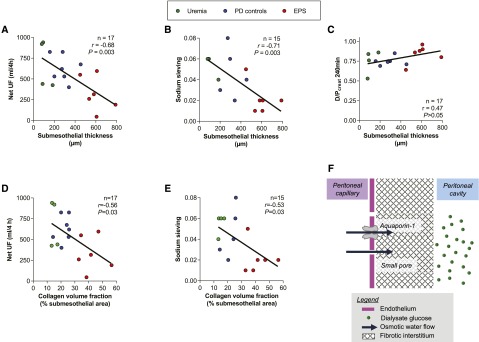
Encapsulating peritoneal sclerosis (EPS) is a rare but severe complication of peritoneal dialysis (PD) characterized by extensive fibrosis of the peritoneum. Changes in peritoneal water transport may precede EPS, but the mechanisms and potential predictive value of that transport defect are unknown. Among 234 patients with ESRD who initiated PD at our institution over a 20-year period, 7 subsequently developed EPS. We evaluated changes in peritoneal transport over time on PD in these 7 patients and in 28 matched controls using 3.86% glucose peritoneal equilibration tests. Compared with long-term PD controls, patients with EPS showed early loss of ultrafiltration capacity and sodium sieving before the onset of overt EPS. Multivariate analysis revealed that loss of sodium sieving was the most powerful predictor of EPS. Compared with long-term PD control and uremic peritoneum, EPS peritoneum showed thicker submesothelial fibrosis, with increased collagen density and a greater amount of thick collagen fibers. Reduced osmotic conductance strongly correlated with the degree of peritoneal fibrosis, but not with vasculopathy. Peritoneal fibrosis was paralleled by an excessive upregulation of vascular endothelial growth factor and endothelial nitric oxide synthase, but the expression of endothelial aquaporin-1 water channels was unaltered. Our findings suggest that an early and disproportionate reduction in osmotic conductance during the course of PD is an independent predictor of EPS. This functional change is linked to specific alterations of the collagen matrix in the peritoneal membrane of patients with EPS, thereby validating the serial three-pore membrane/fiber matrix and distributed models of peritoneal transport.
Keywords: peritoneal dialysis; ultrafiltration; vascular endothelial growth factor; water channels.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Mehrotra R, Chiu YW, Kalantar-Zadeh K, Bargman J, Vonesh E: Similar outcomes with hemodialysis and peritoneal dialysis in patients with end-stage renal disease. Arch Intern Med 171: 110–118, 2011 - PubMed
-
- Davies SJ, Phillips L, Naish PF, Russell GI: Peritoneal glucose exposure and changes in membrane solute transport with time on peritoneal dialysis. J Am Soc Nephrol 12: 1046–1051, 2001 - PubMed
-
- Devuyst O, Margetts PJ, Topley N: The pathophysiology of the peritoneal membrane. J Am Soc Nephrol 21: 1077–1085, 2010 - PubMed
-
- Devuyst O, van Westrhenen R, Topley N: Longterm peritoneal dialysis patients. In: Nolph and Gokal’s Textbook of Peritoneal Dialysis, edited by Khanna R, Krediet RT, 3rd Ed., New York, Springer, 2009, pp 757–780
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
