

N-methyl-D-aspartate receptor antibody-mediated neurological disease: results of a UK-based surveillance study in children
- PMID: 25637141
- PMCID: PMC4453622
- DOI: 10.1136/archdischild-2014-306795
N-methyl-D-aspartate receptor antibody-mediated neurological disease: results of a UK-based surveillance study in children
Abstract
Objective: N-methyl-D-aspartate receptor antibody (NMDAR-Ab) encephalitis is a well-recognised clinico-immunological syndrome that presents with neuropsychiatric symptoms cognitive decline, movement disorder and seizures. This study reports the clinical features, management and neurological outcomes of paediatric NMDAR-Ab-mediated neurological disease in the UK.
Design: A prospective surveillance study. Children with NMDAR-Ab-mediated neurological diseases were voluntarily reported to the British Neurological Surveillance Unit (BPNSU) from November 2010 to December 2011. Initial and follow-up questionnaires were sent out to physicians.
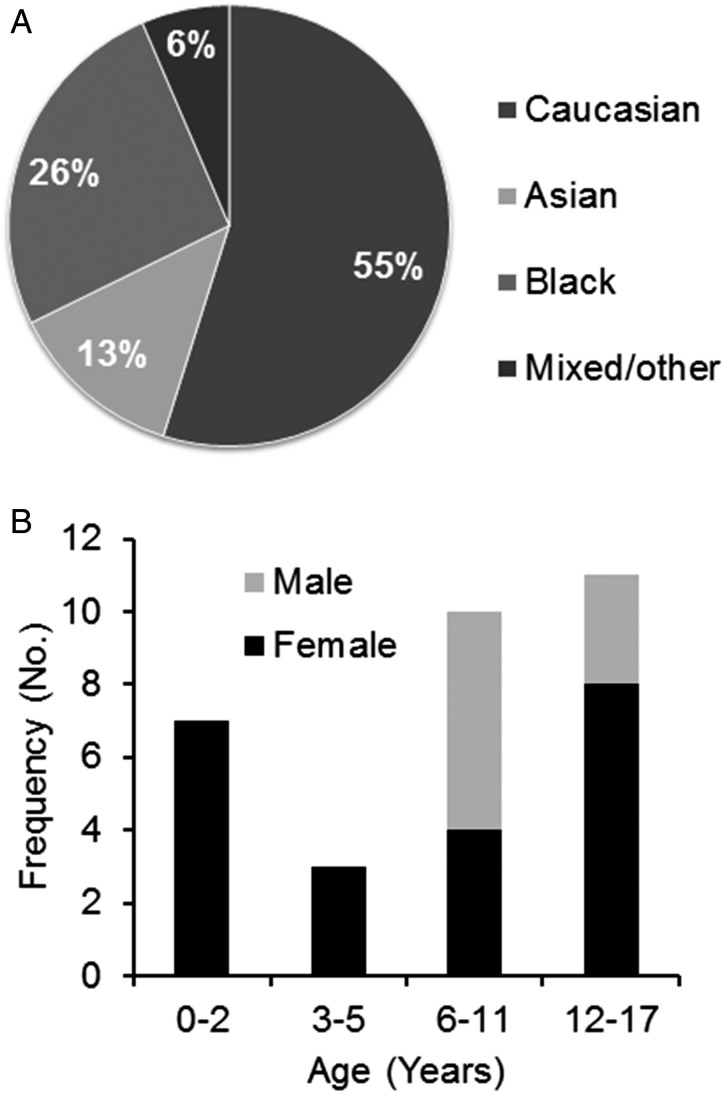
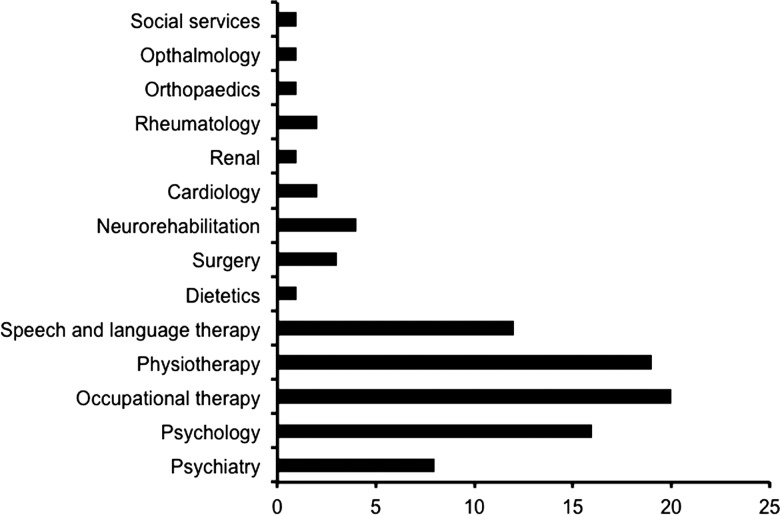
Results: Thirty-one children fulfilled the criteria for the study. Eight presented during the study period giving an incidence of 0.85 per million children per year (95% CI 0.64 to 1.06); 23 cases were historical. Behavioural change and neuropsychiatric features were present in 90% of patients, and seizures and movement disorders both in 67%. Typical NMDAR-Ab encephalitis was reported in 24 children and partial phenotype without encephalopathy in seven, including predominantly psychiatric (four) and movement disorder (three). All patients received steroids, 22 (71%) received intravenous immunoglobulin, 9 (29%) received plasma exchange,and 10 (32%) received second-line immunotherapy. Of the 23 patients who were diagnosed early, 18 (78%) made a full recovery compared with only 1 of 8 (13%) of the late diagnosed patients (p=0.002, Fisher's exact test). Seven patients relapsed, with four needing additional second-line immunotherapy.
Conclusions: Paediatric NMDAR-Ab-mediated neurological disease appears to be similar to adult NMDAR-Ab encephalitis, but some presented with a partial phenotype. Early treatment was associated with a quick and often full recovery.
Keywords: Autoantibody; Encephalitis; NMDA receptors; Neurology; immunotherapy.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures

Comment in
-
Assessing the incidence of anti-NMDAR encephalitis.Arch Dis Child. 2015 Jun;100(6):512-3. doi: 10.1136/archdischild-2014-307978. Epub 2015 Mar 25. Arch Dis Child. 2015. PMID: 25809344 Free PMC article. No abstract available.
References
-
- Vincent A, Bien CG, Irani SR, et al. . Autoantibodies associated with diseases of the CNS: new developments and future challenges. Lancet Neurol 2011;10:759–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical