

Myocardial stiffness in patients with heart failure and a preserved ejection fraction: contributions of collagen and titin
- PMID: 25637629
- PMCID: PMC4390480
- DOI: 10.1161/CIRCULATIONAHA.114.013215
Myocardial stiffness in patients with heart failure and a preserved ejection fraction: contributions of collagen and titin
Abstract
Background: The purpose of this study was to determine whether patients with heart failure and a preserved ejection fraction (HFpEF) have an increase in passive myocardial stiffness and the extent to which discovered changes depend on changes in extracellular matrix fibrillar collagen and cardiomyocyte titin.
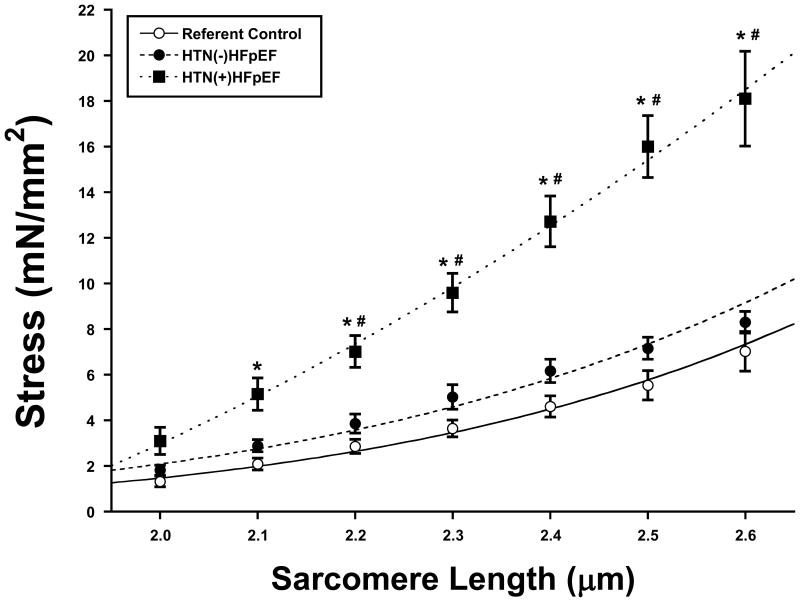
Methods and results: Seventy patients undergoing coronary artery bypass grafting underwent an echocardiogram, plasma biomarker determination, and intraoperative left ventricular epicardial anterior wall biopsy. Patients were divided into 3 groups: referent control (n=17, no hypertension or diabetes mellitus), hypertension (HTN) without (-) HFpEF (n=31), and HTN with (+) HFpEF (n=22). One or more of the following studies were performed on the biopsies: passive stiffness measurements to determine total, collagen-dependent and titin-dependent stiffness (differential extraction assay), collagen assays (biochemistry or histology), or titin isoform and phosphorylation assays. In comparison with controls, patients with HTN(-)HFpEF had no change in left ventricular end-diastolic pressure, myocardial passive stiffness, collagen, or titin phosphorylation but had an increase in biomarkers of inflammation (C-reactive protein, soluble ST2, tissue inhibitor of metalloproteinase 1). In comparison with both control and HTN(-)HFpEF, patients with HTN(+)HFpEF had increased left ventricular end-diastolic pressure, left atrial volume, N-terminal propeptide of brain natriuretic peptide, total, collagen-dependent, and titin-dependent stiffness, insoluble collagen, increased titin phosphorylation on PEVK S11878(S26), reduced phosphorylation on N2B S4185(S469), and increased biomarkers of inflammation.
Conclusions: Hypertension in the absence of HFpEF did not alter passive myocardial stiffness. Patients with HTN(+)HFpEF had a significant increase in passive myocardial stiffness; collagen-dependent and titin-dependent stiffness were increased. These data suggest that the development of HFpEF depends on changes in both collagen and titin homeostasis.
Keywords: collagen; diastole; heart failure; hypertension; hypertrophy.
© 2015 American Heart Association, Inc.
Figures





Comment in
-
Letter by Abu Daya et al Regarding Article, "Myocardial Stiffness in Patients With Heart Failure and a Preserved Ejection Fraction, Contributions of Collagen and Titin".Circulation. 2015 Nov 24;132(21):e248. doi: 10.1161/CIRCULATIONAHA.115.017796. Circulation. 2015. PMID: 26596981 No abstract available.
References
-
- Shah AM, Shah SJ, Anand IS, Sweitzer NK, O'Meara E, Heitner JF, Sopko G, Li G, Assmann SF, McKinlay SM, Pitt B, Pfeffer MA, Solomon SD, TOPCAT Investigators Cardiac structure and function in heart failure with preserved ejection fraction: baseline findings from the echocardiographic study of the treatment of preserved cardiac function heart failure with an aldosterone antagonist trial. Circ Heart Fail. 2014;7:104–15. - PMC - PubMed
-
- Zile MR, Gottdiener JS, Hetzel SJ, McMurray JJ, Komajda M, McKelvie R, Baicu CF, Massie BM, Carson PE. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation. 2011;124:2491–2501. - PubMed
-
- Zile MR, Bennett TD, John Sutton M, Cho YK, Adamson PB, Aaron MF, Aranda JM, Jr, Abraham WT, Smart FW, Warner-Stevenson L, Kueffer FJ, Bourge RC. Transition from chronic compensated to acute decompensated heart failure: pathophysiologic insights obtained from continuous monitoring of intracardiac pressures. Circulation. 2008;118:1433–1441. - PubMed
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure-abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–9. - PubMed
-
- Zile MR, Gaasch WH, Carroll JD, Feldman MD, Aurigemma GP, Schaer GL, Ghali JK, Liebson PR. Heart failure with a normal ejection fraction. Is measurement of diastolic function necessary to make the diagnosis of diastolic heart failure? Circulation. 2001;104:779–782. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R56HL123478/HL/NHLBI NIH HHS/United States
- R56 HL123478/HL/NHLBI NIH HHS/United States
- R01HL089944/HL/NHLBI NIH HHS/United States
- U10 HL110342/HL/NHLBI NIH HHS/United States
- UL1TR000062/TR/NCATS NIH HHS/United States
- R01 HL123478/HL/NHLBI NIH HHS/United States
- R01 HL115988/HL/NHLBI NIH HHS/United States
- UL1 TR000062/TR/NCATS NIH HHS/United States
- I01 CX000415/CX/CSRD VA/United States
- R01 HL122744/HL/NHLBI NIH HHS/United States
- R01HL06288/HL/NHLBI NIH HHS/United States
- R01 HL118524/HL/NHLBI NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- U10 HL110302/HL/NHLBI NIH HHS/United States
- R01 HL089944/HL/NHLBI NIH HHS/United States
- I01 BX000487/BX/BLRD VA/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
