

Pharmacokinetic model of unfractionated heparin during and after cardiopulmonary bypass in cardiac surgery
- PMID: 25638272
- PMCID: PMC4326208
- DOI: 10.1186/s12967-015-0404-5
Pharmacokinetic model of unfractionated heparin during and after cardiopulmonary bypass in cardiac surgery
Abstract
Background: Unfractionated heparin (UFH) is widely used as a reversible anti-coagulant in cardiopulmonary bypass (CPB). However, the pharmacokinetic characteristics of UFH in CPB surgeries remain unknown because of the lack of means to directly determine plasma UFH concentrations. The aim of this study was to establish a pharmacokinetic model to predict plasma UFH concentrations at the end of CPB for optimal neutralization with protamine sulfate.
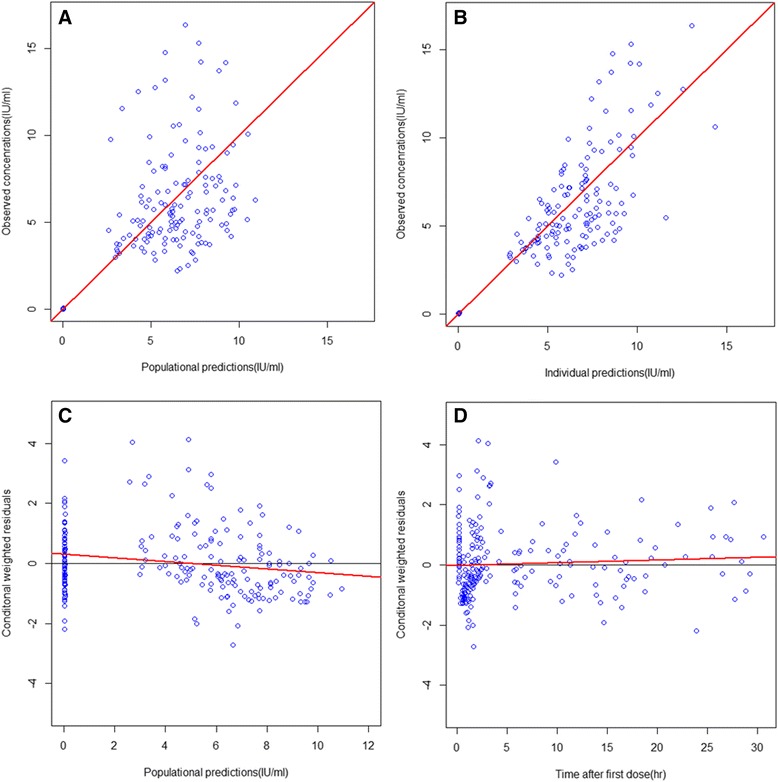
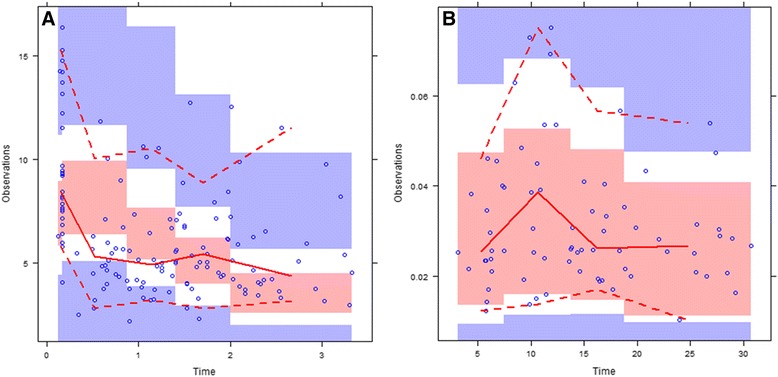
Methods: Forty-one patients undergoing CPB during cardiac surgery were enrolled in this observational clinical study of UFH pharmacokinetics. Patients received intravenous injections of UFH, and plasma anti-FIIa activity was measured with commercial anti-FIIa assay kits. A population pharmacokinetic model was established by using nonlinear mixed-effects modeling (NONMEM) software and validated by visual predictive check and Bootstrap analyses. Estimated parameters in the final model were used to simulate additional protamine administration after cardiac surgery in order to eliminate heparin rebound. Plans for postoperative protamine intravenous injections and infusions were quantitatively compared and evaluated during the simulation.
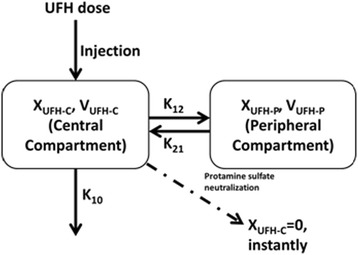
Results: A two-compartment pharmacokinetic model with first-order elimination provided the best fit. Subsequent simulation of postoperative protamine administration suggested that a lower-dose protamine infusion over 24 h may provide better elimination and prevent heparin rebound than bolus injection and other infusion regimens that have higher infusion rates and shorter duration.
Conclusion: A two-compartment model accurately reflects the pharmacokinetics of UFH in Chinese patients during CPB and can be used to explain postoperative heparin rebound after protamine neutralization. Simulations suggest a 24-h protamine infusion is more effective for heparin rebound prevention than a 6-h protamine infusion.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
