

Age-related changes to cardiac systolic and diastolic function during whole-body passive hyperthermia
- PMID: 25641368
- PMCID: PMC4948727
- DOI: 10.1113/expphysiol.2014.083014
Age-related changes to cardiac systolic and diastolic function during whole-body passive hyperthermia
Abstract
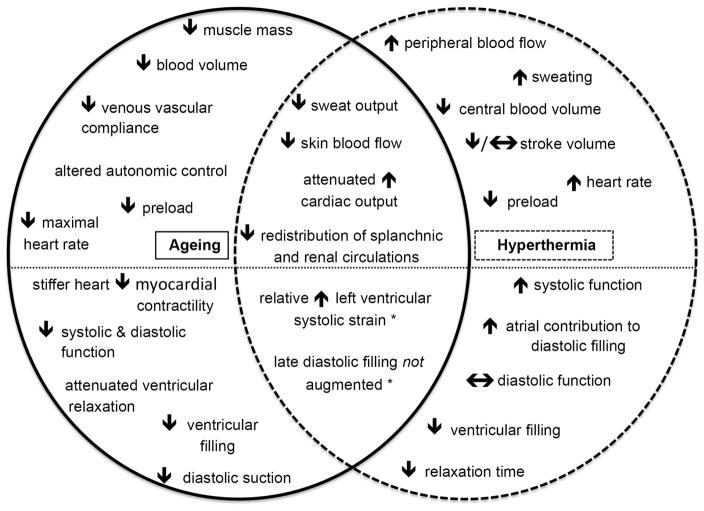
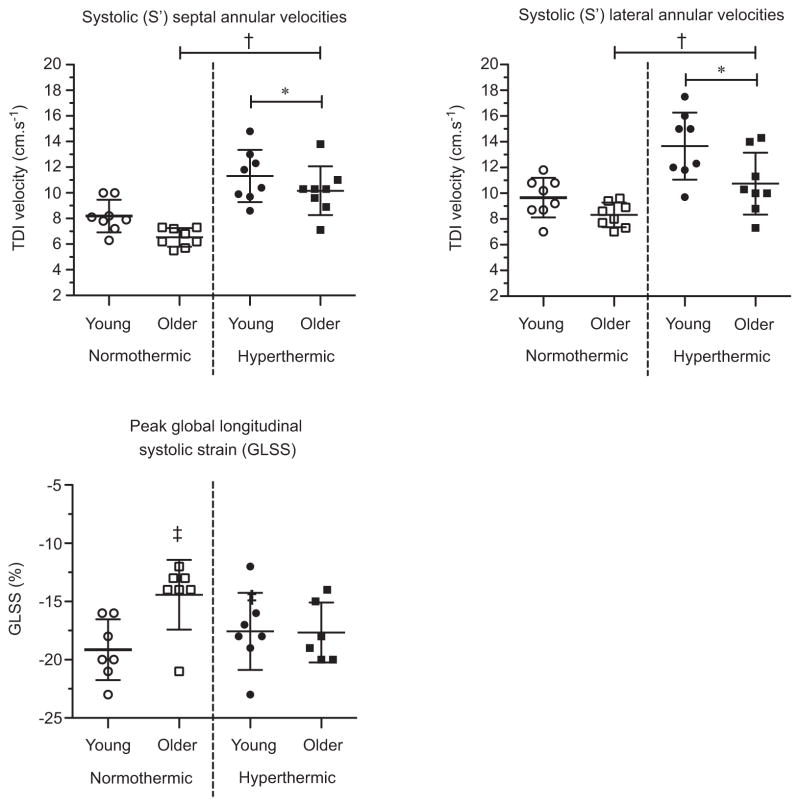
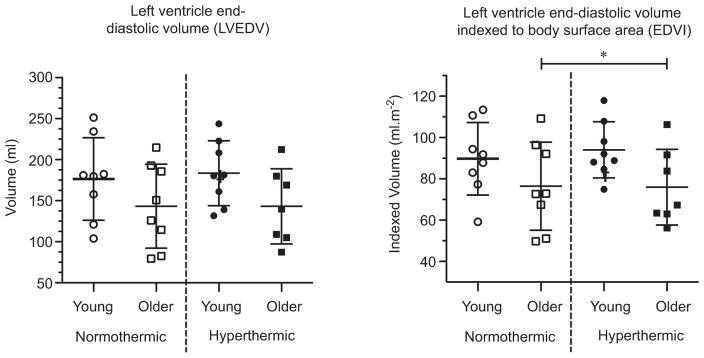
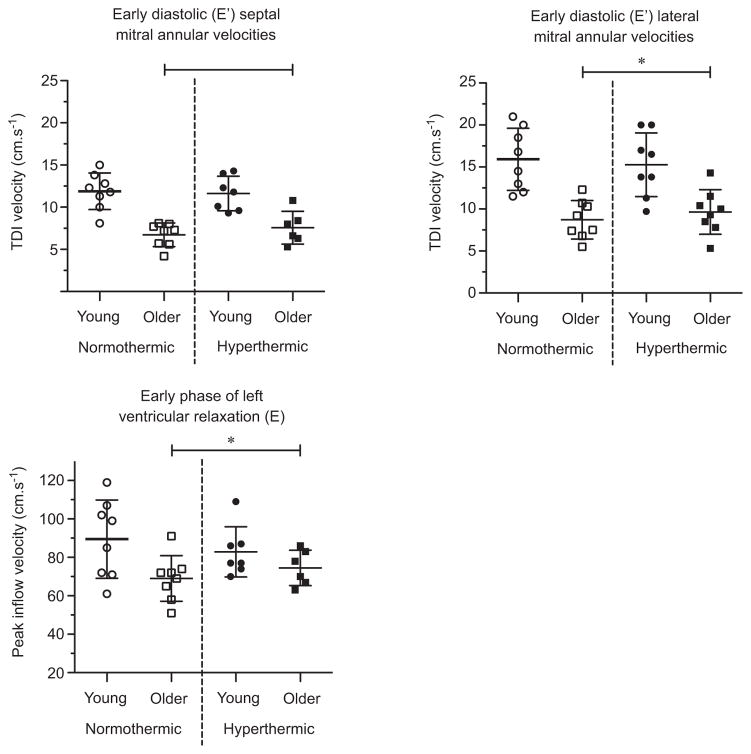
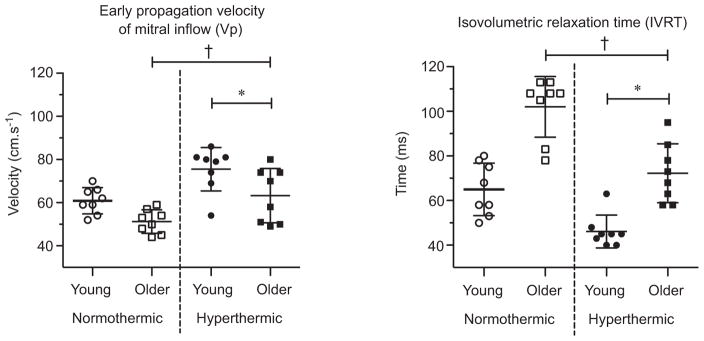
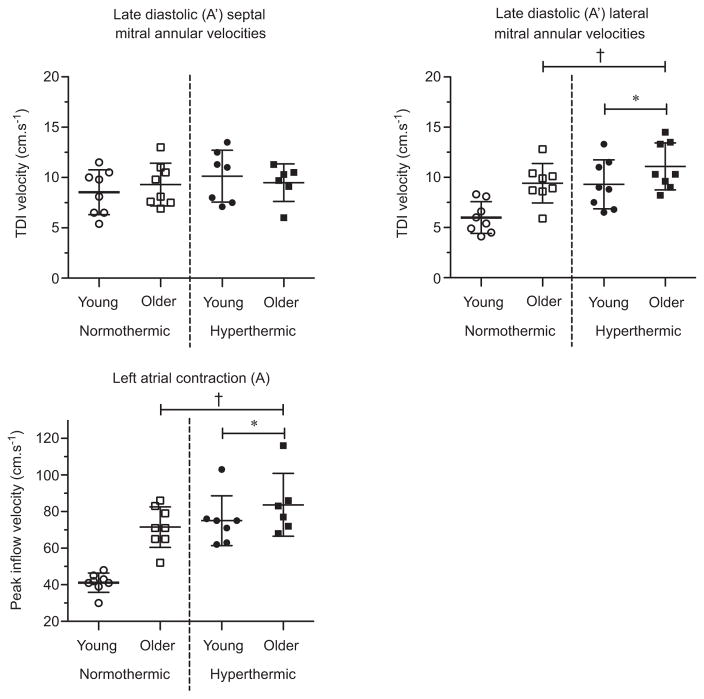
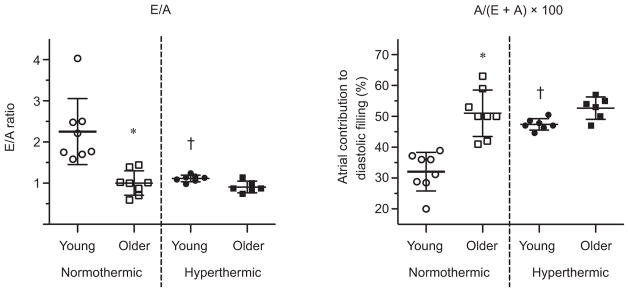
What is the central question of this study? The effect of ageing on hyperthermia-induced changes in cardiac function is unknown. What is the main finding and its importance? Using echocardiography, we show that during hyperthermia the systolic and diastolic function can be appropriately augmented to meet cardiac demand in healthy older adults, although overall age-related impairments remain. One exception was late diastolic ventricular filling [i.e. E/A ratio and A/(A + E) ratio], which in the older adults was not further augmented during hyperthermia, unlike their young counterparts. To meet cardiac demand, therefore, healthy older adults appear to depend on an increased left ventricular systolic strain and proportion of their cardiac reserve. The effect of ageing on hyperthermia-induced changes in cardiac function is unknown. This study tested the hypothesis that hyperthermia-induced changes in left ventricular systolic and diastolic function are attenuated in older adults when compared with young adults. Eight older (71 ± 5 years old) and eight young adults (29 ± 5 years old), matched for sex, physical activity and body mass index, underwent whole-body passive hyperthermia. Mean arterial pressure (Finometer Pro), heart rate, forearm vascular conductance (venous occlusion plethysmography) and echocardiographic indices of diastolic and systolic function were measured during a normothermic supine period and again after an increase in internal temperature of ∼1.0 °C. Hyperthermia decreased mean arterial pressure and left ventricular end-diastolic volumes and increased heart rate to a similar extent in both groups (P > 0.05). Ageing did not alter the magnitude of hyperthermia-induced changes in indices of systolic (lateral mitral annular S' velocity) or diastolic function (lateral mitral annular E' velocity, peak early diastolic filling and isovolumic relaxation time; P > 0.05). However, with hyperthermia the global longitudinal systolic strain increased in the older group, but was unchanged in the young group (P = 0.03). Also, older adults were unable to augment late diastolic ventricular filling [i.e. E/A ratio and A/(A + E) ratio] during hyperthermia, unlike the young (P < 0.05). These findings indicate that older adults depend on a greater systolic contribution (global longitudinal systolic strain) to meet hyperthermic demand and that the atrial contribution to diastolic filling was not further augmented in older adults when compared with young adults.
© 2015 The Authors. Experimental Physiology © 2015 The Physiological Society.
Conflict of interest statement
None declared.
Figures
References
-
- Agostoni P, Cattadori G, Apostolo A, Contini M, Palermo P, Marenzi G, Wasserman K. Noninvasive measurement of cardiac output during exercise by inert gas rebreathing technique: a new tool for heart failure evaluation. J Am Coll Cardiol. 2005;46:1779–1781. - PubMed
-
- Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, Thomas JD, Palmer D, Levine BD. Effect of aging and physical activity on left ventricular compliance. Circulation. 2004;110:1799–1805. - PubMed
-
- Armstrong CG, Kenney WL. Effects of age and acclimation on responses to passive heat exposure. J Appl Physiol. 1993;75:2162–2167. - PubMed
-
- Åström DO, Forsberg B, Rocklöv J. Heat wave impact on morbidity and mortality in the elderly population: a review of recent studies. Maturitas. 2011;69:99–105. - PubMed
-
- Basu R, Samet JM. Relation between elevated ambient temperature and mortality: a review of the epidemiologic evidence. Epidemiol Rev. 2002;24:190–202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical