

Balancing the risks of bleeding and stent thrombosis: a decision analytic model to compare durations of dual antiplatelet therapy after drug-eluting stents
- PMID: 25641531
- PMCID: PMC4407277
- DOI: 10.1016/j.ahj.2014.11.002
Balancing the risks of bleeding and stent thrombosis: a decision analytic model to compare durations of dual antiplatelet therapy after drug-eluting stents
Abstract
Background: After coronary stent placement, whether dual antiplatelet therapy (DAPT) duration should be extended to prevent late stent thrombosis (ST) or adverse cardiovascular events is uncertain.
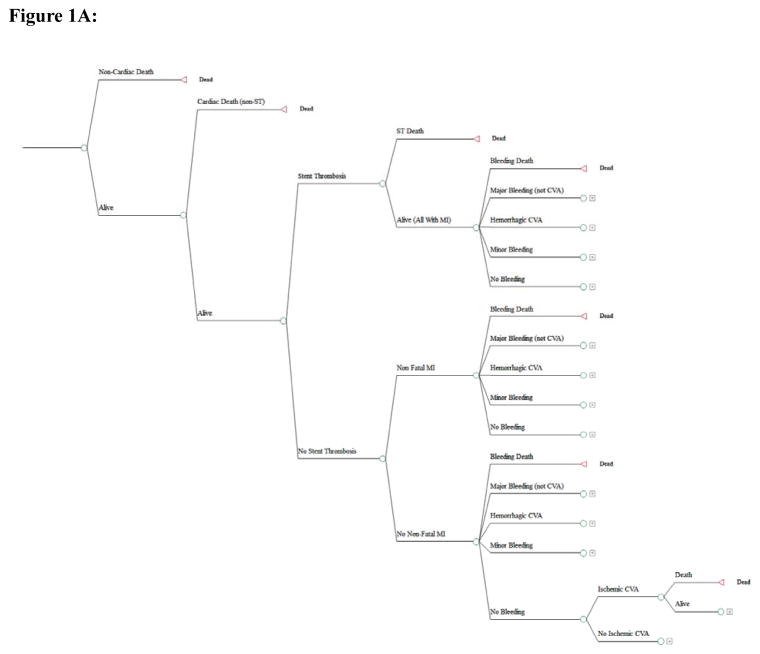
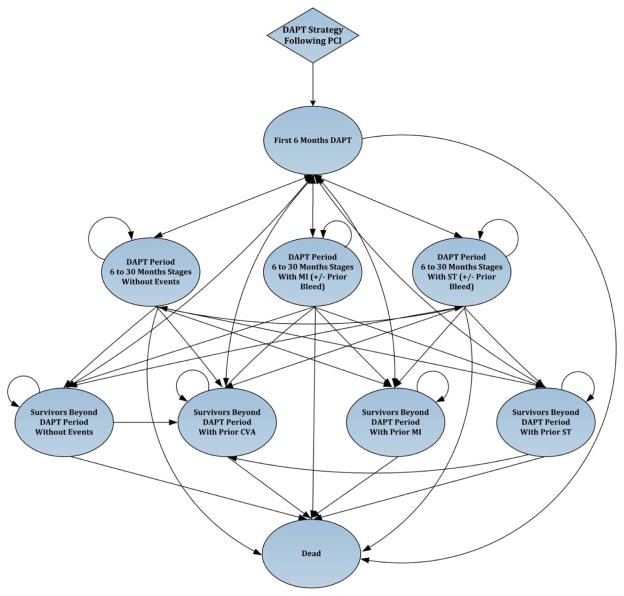
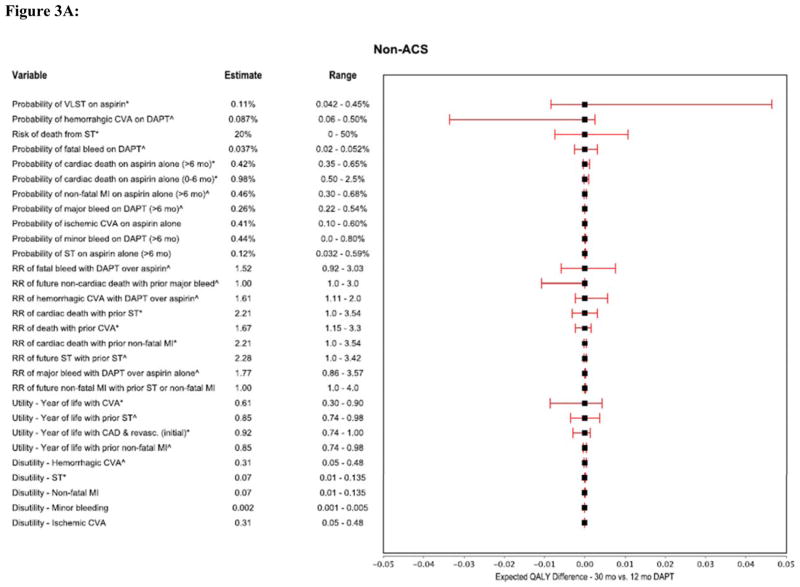
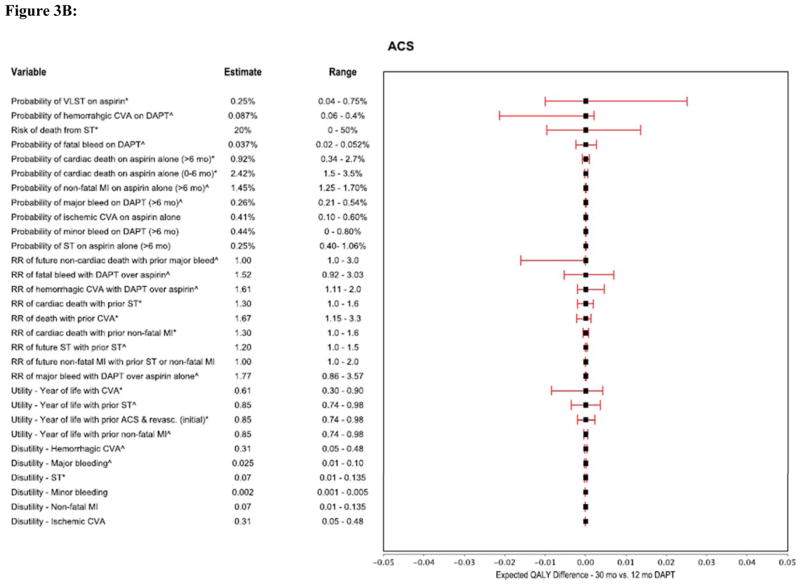
Methods: To define the reduction in ischemic events required to outweigh increased bleeding with longer-duration DAPT, we developed a decision-analytic Markov model comparing DAPT durations of 6, 12, and 30 months after DES. Separate models were developed for patients presenting with and without an acute coronary syndrome (ACS). We used sensitivity analyses to identify the incremental benefit of longer-duration DAPT on either ST or the composite of cardiac death, myocardial infarction, and ischemic stroke (major adverse cardiovascular and cerebrovascular events [MACCEs]) required to outweigh the increased risk of bleeding associated with longer DAPT. The outcome from each strategy was quantified in terms of quality-adjusted life years.
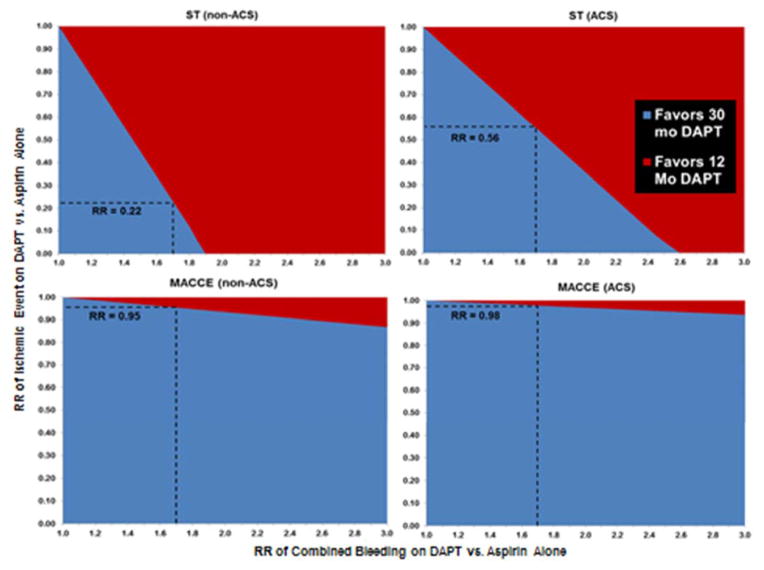
Results: In the non-ACS population, in order for 30 months of DAPT to be preferred over 12 months of therapy, DAPT would have to result in a 78% reduction in the risk of ST (relative risk [RR] 0.22, 3.1 fewer events per 1000) and only a 5% reduction in MACCE (RR 0.95, 2.2 fewer events per 1000) as compared with aspirin alone. For the ACS population, DAPT would have to result in a 44% reduction in the risk of ST (RR 0.56, 3.4 fewer events per 1000) but only a 2% reduction in MACCE (RR 0.98, 2.3 fewer events per 1000) as compared with aspirin alone, for 30 months of DAPT to be preferred for 12 months.
Conclusions: Small absolute differences in the risk of ischemic events with longer DAPT would be sufficient to outweigh the known bleeding risks.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Palmerini T, Biondi-Zoccai G, Della Riva D, Stettler C, Sangiorgi D, D'Ascenzo F, Kimura T, Briguori C, Sabate M, Kim HS, De Waha A, Kedhi E, Smits PC, Kaiser C, Sardella G, Marullo A, Kirtane AJ, Leon MB, Stone GW. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet. 2012;379:1393–1402. - PubMed
-
- Mauri L, Hsieh WH, Massaro JM, Ho KK, D'Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356:1020–1029. - PubMed
-
- Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G, Airoldi F, Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N, Briguori C, Gerckens U, Grube E, Colombo A. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293:2126–2130. - PubMed
-
- Cutlip DE, Baim DS, Ho KK, Popma JJ, Lansky AJ, Cohen DJ, Carrozza JP, Jr, Chauhan MS, Rodriguez O, Kuntz RE. Stent thrombosis in the modern era: A pooled analysis of multicenter coronary stent clinical trials. Circulation. 2001;103:1967–1971. - PubMed
-
- Bhatt DL, Fox KA, Hacke W, Berger PB, Black HR, Boden WE, Cacoub P, Cohen EA, Creager MA, Easton JD, Flather MD, Haffner SM, Hamm CW, Hankey GJ, Johnston SC, Mak KH, Mas JL, Montalescot G, Pearson TA, Steg PG, Steinhubl SR, Weber MA, Brennan DM, Fabry-Ribaudo L, Booth J, Topol EJ. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354:1706–1717. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
