

Suboptimal compliance with surgical safety checklists in Colorado: A prospective observational study reveals differences between surgical specialties
- PMID: 25642287
- PMCID: PMC4312457
- DOI: 10.1186/s13037-014-0056-z
Suboptimal compliance with surgical safety checklists in Colorado: A prospective observational study reveals differences between surgical specialties
Abstract
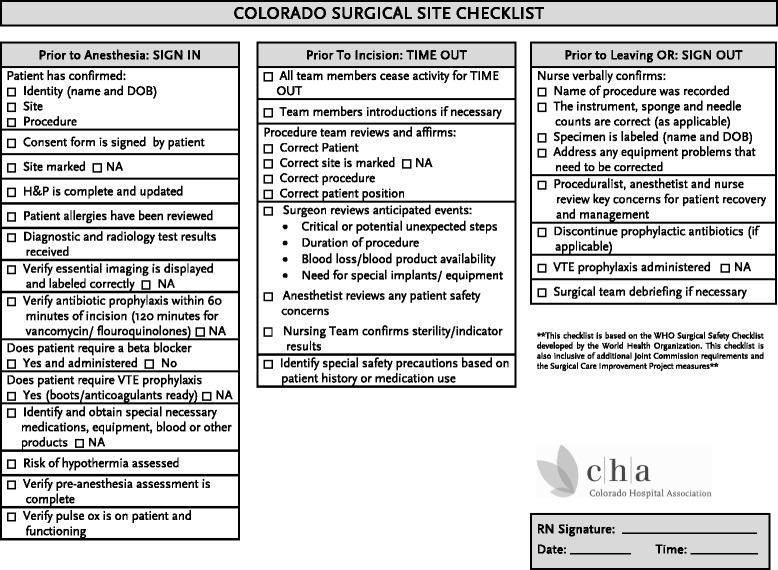
Background: Surgical safety checklists (SSCs) are designed to improve team communication and consistency in care, ultimately avoiding complications. In Colorado, hospitals reported that use of SSCs was standard practice, but a statewide survey indicated that SSC use was inconsistent. The purpose of this project was to directly observe the compliance with the SSC in Colorado hospitals, through direct observation of the perioperative checklist process.
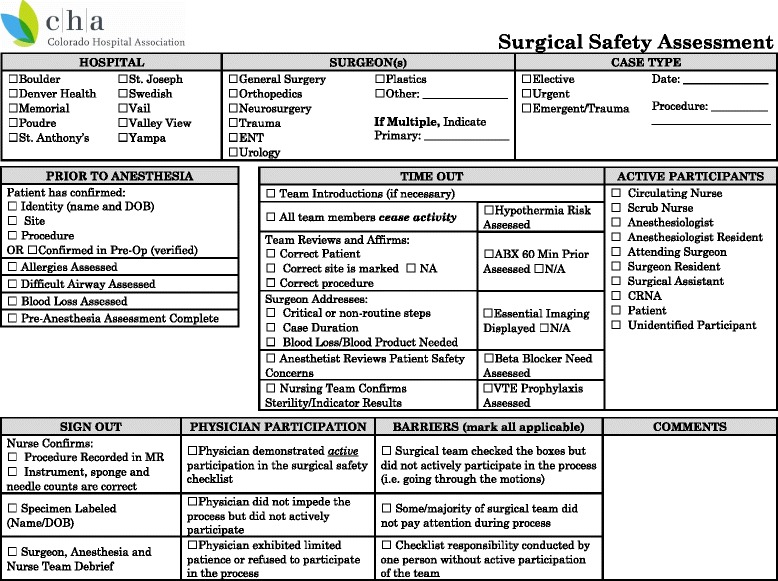
Methods: Ten hospitals participated in a quality improvement initiative. Trained team members recorded compliance with each of the components of the SSC. Data analysis was performed using a chi-squared test or ANOVA, depending on the number of categorical variables, with p < 0.05 determining statistical significance.
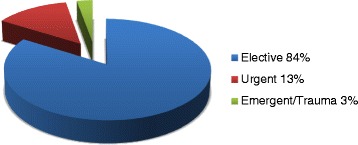
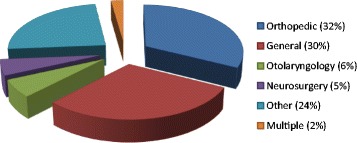
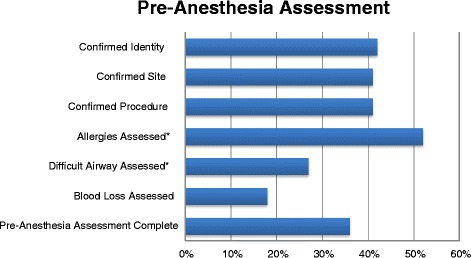
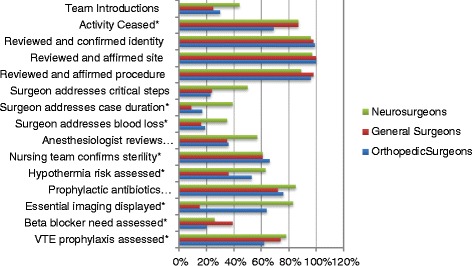
Results: Ten hospitals representing statewide diversity submitted 854 observations (median 98, range 24-106). 83% of cases were elective, 13% urgent, and 4% emergent/trauma. There was significant variation across hospitals in: team introductions, cessation of activity, affirming correct procedure, assessing hypothermia risk, need for beta blocker, or VTE prophylaxis. Uniformly poor compliance was observed with respect to assessment of case duration, blood loss, anesthesiologists' concerns, or display of essential imaging. Only 71% of observers reported active participation by physicians; 9% reported that "the majority did not pay attention" and 4% reported that the team was "just going through the motions". There were significant differences among surgical specialty groups in the majority of the elements.
Conclusion: SSCs have been implemented by the vast majority of hospitals in our state; however, compliance with SSC completion in the operating room has wide variation and is generally suboptimal. Although this study was not designed to correlate SSC compliance with outcomes, there are concerns about the risk of a sentinel event or unanticipated complication resulting from poor preparation.
Keywords: Checklist; Compliance; Implementation; Observation; Operating room; Safety; Sentinel events; Surgeons; Surgery.
Figures

Similar articles
-
A quality improvement initiative using peer audit and feedback to improve compliance.Int J Qual Health Care. 2022 Jul 15;34(3):mzac058. doi: 10.1093/intqhc/mzac058. Int J Qual Health Care. 2022. PMID: 35770658 Free PMC article.
-
Attitudes and compliance with the WHO surgical safety checklist: a survey among surgeons and operating room staff in 138 hospitals in China.Patient Saf Surg. 2021 Jan 6;15(1):3. doi: 10.1186/s13037-020-00276-0. Patient Saf Surg. 2021. PMID: 33407718 Free PMC article.
-
Implementation of the Surgical Safety Checklist in South Carolina Hospitals Is Associated with Improvement in Perceived Perioperative Safety.J Am Coll Surg. 2016 May;222(5):725-736.e5. doi: 10.1016/j.jamcollsurg.2015.12.052. Epub 2016 Jan 13. J Am Coll Surg. 2016. PMID: 27049781
-
Facilitators and barriers to the implementation of surgical safety checklist: an integrative review.Int J Qual Health Care. 2023 Oct 31;35(4):mzad086. doi: 10.1093/intqhc/mzad086. Int J Qual Health Care. 2023. PMID: 37847116 Review.
-
Development of an Enhanced Recovery After Surgery Surgical Safety Checklist Through a Modified Delphi Process.JAMA Netw Open. 2023 Feb 1;6(2):e2248460. doi: 10.1001/jamanetworkopen.2022.48460. JAMA Netw Open. 2023. PMID: 36753283
Cited by
-
Improving the WHO Surgical Safety Checklist sign-out.BJS Open. 2021 May 7;5(3):zrab028. doi: 10.1093/bjsopen/zrab028. BJS Open. 2021. PMID: 33960366 Free PMC article.
-
Surgical provider-reported reasons for utilization of the World Health Organization's Surgical Safety Checklist at a tertiary hospital in Ghana.PLOS Glob Public Health. 2023 Jan 12;3(1):e0001143. doi: 10.1371/journal.pgph.0001143. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 36962845 Free PMC article.
-
Surgeons, sign your site!Patient Saf Surg. 2017 Apr 4;11:8. doi: 10.1186/s13037-017-0122-4. eCollection 2017. Patient Saf Surg. 2017. PMID: 28392833 Free PMC article.
-
The role of teamwork and non-technical skills for improving emergency surgical outcomes: an international perspective.Patient Saf Surg. 2022 Feb 8;16(1):8. doi: 10.1186/s13037-022-00317-w. Patient Saf Surg. 2022. PMID: 35135584 Free PMC article. Review.
-
The antibiotic checklist: an observational study of the discrepancy between reported and actually performed checklist items.BMC Infect Dis. 2018 Jan 8;18(1):16. doi: 10.1186/s12879-017-2878-7. BMC Infect Dis. 2018. PMID: 29310569 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
