

Unmet contraceptive needs among refugees
Abstract
Objective: To describe what women of reproductive age who received primary care at a refugee health clinic were using for contraception upon arrival to the clinic, and to quantify the unmet contraceptive needs within that population.
Design: Retrospective chart review.
Setting: Crossroads Clinic in downtown Toronto, Ont.
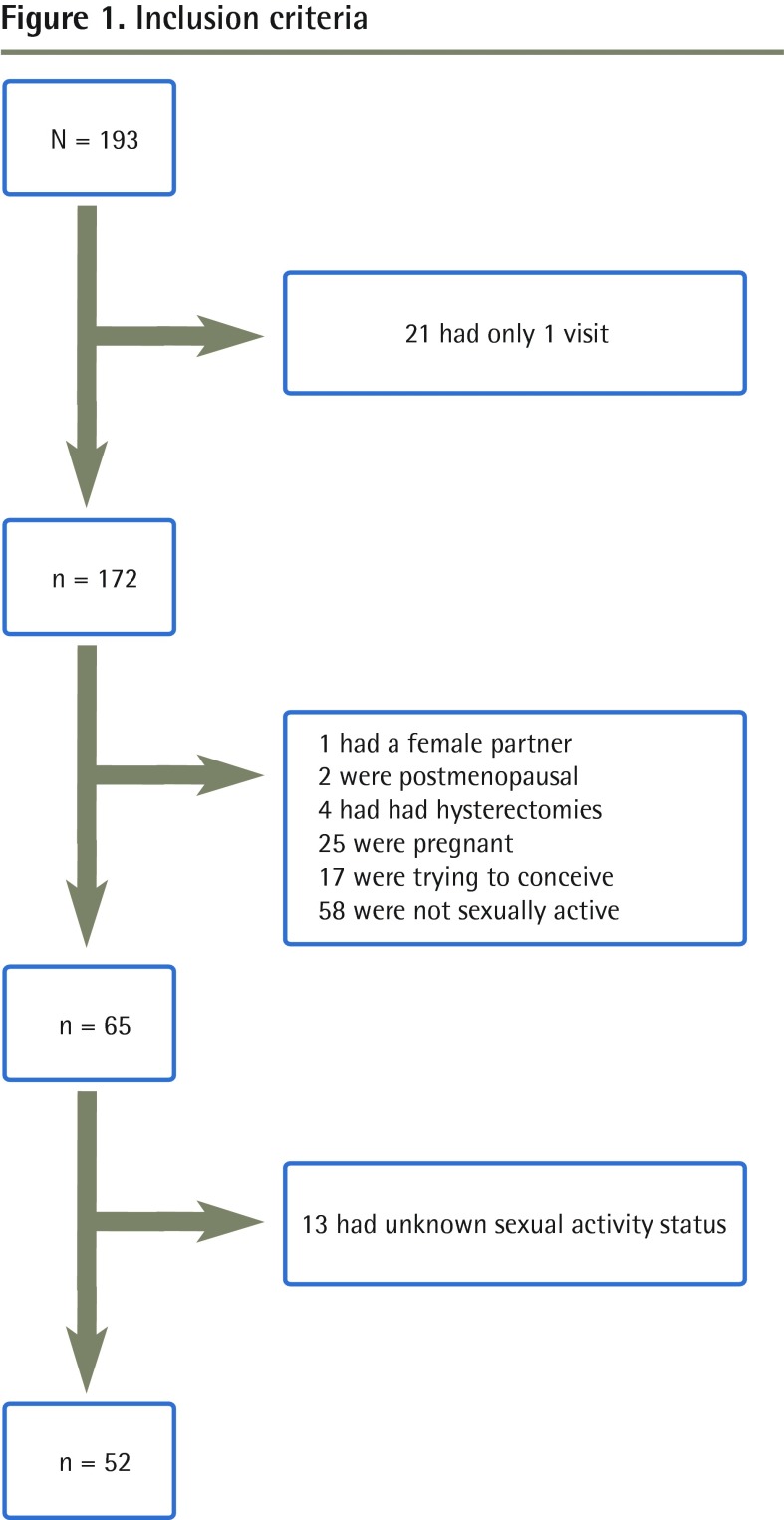
Participants: Women of reproductive age (15 to 49 years) who first presented for care between December 1, 2011, and December 1, 2012. To be included, a woman had to have had 2 or more clinic visits or an annual health examination. Exclusion criteria for the contraception prevalence calculation were female sexual partner, menopause, hysterectomy, pregnancy, or trying to conceive.
Main outcome measures: Contraception use prevalence was measured, as was unmet contraceptive need, which was calculated using a modified version of the World Health Organization's definition: the number of women with an unmet need was expressed as a percentage of women of reproductive age who were married or in a union, or who were sexually active.
Results: Overall, 52 women met the criteria for inclusion in the contraceptive prevalence calculation. Of these, 16 women (30.8%) did not use any form of contraception. Twelve women were pregnant at some point in the year and stated the pregnancy was unwanted or mistimed. An additional 14 women were not using contraception but had no intention of becoming pregnant within the next 2 years. There were no women with postpartum amenorrhea not using contraception and who had wanted to delay or prevent their previous pregnancy. In total, 97 women were married or in a union, or were sexually active. Unmet need was calculated as follows: (12 + 14 + 0)/97 = 26.8%.
Conclusion: There was a high unmet contraceptive need in the refugee population in our study. All women of reproductive age should be screened for contraceptive need when first seeking medical care in Canada.
Objectif: Déterminer lesquelles parmi les femmes en âge de procréer qui reçoivent des soins primaires à une clinique de santé pour réfugiés utilisaient une méthode contraceptive à leur arrivée à la clinique et quantifier leur taux de besoins de contraception non satisfaits.
Type d’étude: Revue rétrospective de dossiers.
Contexte: La clinique Crossroads du centre-ville de Toronto, en Ontario.
Participantes: Des femmes en âge de procréer de 15 à 49 ans ayant consulté pour la première fois entre le 1er décembre 2011 et le 1er décembre 2012. Pour être incluse, une femme devait avoir visité la clinique au moins 2 fois ou y avoir eu un examen de santé annuel. Les critères d’exclusion suivants ont été utilisés pour le calcul de la prévalence de contraception : avoir une femme comme partenaire sexuelle, être ménopausée, avoir eu une hystérectomie, être enceinte ou chercher à le devenir.
Principaux paramètres à l’étude: La prévalence d’utilisation d’une méthode contraceptive; le taux de besoins de contraception non satisfaits, calculé à l’aide d’une version modifiée de la définition de l’Organisation mondiale de la Santé, c’est-à-dire en exprimant le nombre de femmes ayant des besoins non satisfaits en pourcentage des femmes en âge de procréer qui étaient mariées ou en union libre, ou qui étaient sexuellement actives.
Résultats: En tout, 52 femmes ont répondu aux critères d’inclusion pour le calcul de la prévalence de contraception. Parmi ces femmes, 16 (30,8 %) n’utilisaient aucune méthode contraceptive. À un moment ou l’autre de l’année, 12 femmes ont été enceintes et ont déclaré que leur grossesse n’était pas désirée ou survenait à un mauvais moment. Un autre groupe de 14 femmes n’utilisaient pas de contraception alors qu’elles n’avaient aucune intention de devenir enceintes au cours des 2 années suivantes. Les femmes en aménorrhée du postpartum à la suite d’une grossesse non désirée ou survenue à un moment inopportun utilisaient toutes une méthode contraceptive (nombre de ces femmes n’utilisant pas de méthode = 0). Au total, 97 femmes étaient mariées, en union libre ou étaient sexuellement actives. On s’est servi du nombre de femmes dans chacun de ces groupes pour calculer le taux de besoins non satisfaits: (12 + 14 + 0) ÷ 97 = 26,8 %.
Conclusion: Cette étude a permis de constater qu’il y a beaucoup de besoins de contraception non satisfaits chez les réfugiés. On devrait aborder le sujet de la contraception avec toutes les femmes en âge de procréer qui consultent pour la première fois au Canada.
Figures
Similar articles
-
Unmet family planning needs among female refugees and asylum seekers in Germany - is free access to family planning services enough? Results of a cross-sectional study.Reprod Health. 2020 Jul 29;17(1):115. doi: 10.1186/s12978-020-00962-3. Reprod Health. 2020. PMID: 32727500 Free PMC article.
-
Contraceptive use and unmet need for family planning in Iran.Int J Gynaecol Obstet. 2013 May;121(2):157-61. doi: 10.1016/j.ijgo.2012.11.024. Epub 2013 Mar 6. Int J Gynaecol Obstet. 2013. PMID: 23473347
-
Intention to use contraceptives and subsequent contraceptive behavior in Morocco.Stud Fam Plann. 1996 Sep-Oct;27(5):239-50. Stud Fam Plann. 1996. PMID: 8923652
-
The causes of unmet need for contraception and the social content of services.Stud Fam Plann. 1995 Mar-Apr;26(2):57-75. Stud Fam Plann. 1995. PMID: 7618196 Review.
-
Meeting unmet need: new strategies.Popul Rep J. 1996 Sep;(43):1-35. Popul Rep J. 1996. PMID: 8948001 Review.
Cited by
-
Overcoming the Challenges Faced by Immigrant Populations While Accessing Primary Care: Potential Solution-oriented Actions Advocated by the Bangladeshi-Canadian Community.J Prim Care Community Health. 2021 Jan-Dec;12:21501327211010165. doi: 10.1177/21501327211010165. J Prim Care Community Health. 2021. PMID: 33882748 Free PMC article.
-
Unmet Healthcare Needs Among Migrant Populations in Canada: Exploring the Research Landscape Through a Systematic Integrative Review.J Immigr Minor Health. 2021 Apr;23(2):353-372. doi: 10.1007/s10903-020-01086-3. Epub 2020 Sep 26. J Immigr Minor Health. 2021. PMID: 32979131
-
Household income and contraceptive methods among female youth: a cross-sectional study using the Canadian Community Health Survey (2009-2010 and 2013-2014).CMAJ Open. 2019 Nov 4;7(4):E646-E653. doi: 10.9778/cmajo.20190087. Print 2019 Oct-Dec. CMAJ Open. 2019. PMID: 31690652 Free PMC article.
-
"In Africa, There Was No Family Planning. Every Year You Just Give Birth": Family Planning Knowledge, Attitudes, and Practices Among Somali and Congolese Refugee Women After Resettlement to the United States.Qual Health Res. 2020 Feb;30(3):391-408. doi: 10.1177/1049732319861381. Epub 2019 Jul 26. Qual Health Res. 2020. PMID: 31347453 Free PMC article.
-
Determinants of modern contraceptive use among married Somali women living in Kampala; a cross sectional survey.Reprod Health. 2020 May 24;17(1):72. doi: 10.1186/s12978-020-00922-x. Reprod Health. 2020. PMID: 32448285 Free PMC article.
References
-
- Office of the United Nations High Commissioner for Human Rights, World Health Organization. The right to health. Fact sheet no. 31. Geneva, Switz: United Nations; 2008. Available from: www.ohchr.org/Documents/Publications/Factsheet31.pdf. Accessed 2014 Nov 11.
-
- United Nations Millennium Development Goals [website] Goal 5: improve maternal health. Geneva, Switz: United Nations; 2013. Available from: www.un.org/millenniumgoals/maternal.shtml/. Accessed 2014 Nov 11.
-
- United Nations Population Fund. Key issues in reproductive health services. New York, NY: United Nations Population Fund; 2012.
-
- World Health Organization [website] Health topics. Reproductive health. Geneva, Switz: World Health Organization; 2013. Available from: www.who.int/topics/reproductive_health/en/. Accessed 2014 Nov 25.
-
- Guttmacher Institute, United Nations Population Fund. Fact sheet. Costs and benefits of investing in contraceptive services in the developing world. New York, NY: Guttmacher Institute; 2012.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous