

Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis
- PMID: 25643002
- PMCID: PMC4388802
- DOI: 10.1001/jamainternmed.2014.7779
Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis
Erratum in
-
Error in figures.JAMA Intern Med. 2015 Apr;175(4):659. doi: 10.1001/jamainternmed.2015.0994. JAMA Intern Med. 2015. PMID: 25844755 No abstract available.
Abstract
Importance: Delirium, an acute disorder with high morbidity and mortality, is often preventable through multicomponent nonpharmacological strategies. The efficacy of these strategies for preventing subsequent adverse outcomes has been limited to small studies to date.
Objective: To evaluate available evidence on multicomponent nonpharmacological delirium interventions in reducing incident delirium and preventing poor outcomes associated with delirium.
Data sources: PubMed, Google Scholar, ScienceDirect, and the Cochrane Database of Systematic Reviews from January 1, 1999, to December 31, 2013.
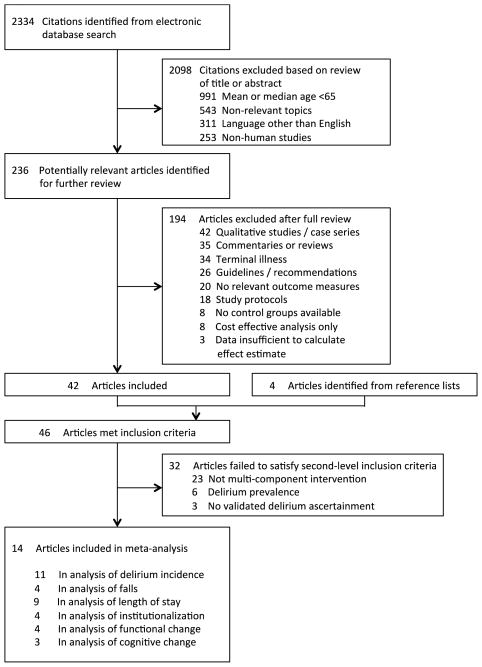
Study selection: Studies examining the following outcomes were included: delirium incidence, falls, length of stay, rate of discharge to a long-term care institution (institutionalization), and change in functional or cognitive status.
Data extraction and synthesis: Two experienced physician reviewers independently and blindly abstracted data on outcome measures using a standardized approach. The reviewers conducted quality ratings based on the Cochrane risk-of-bias criteria for each study.
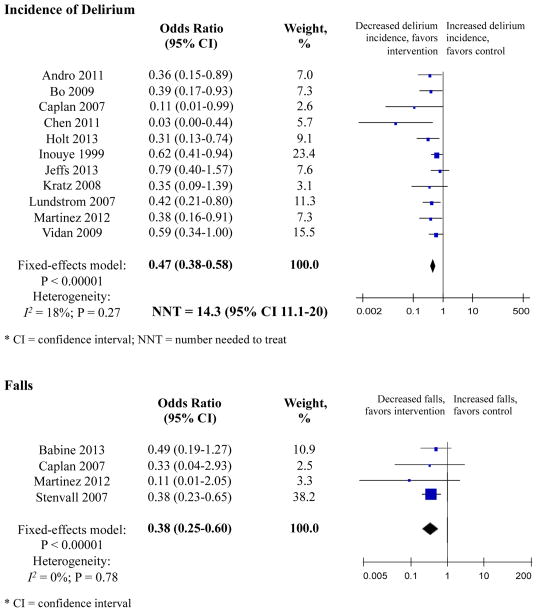
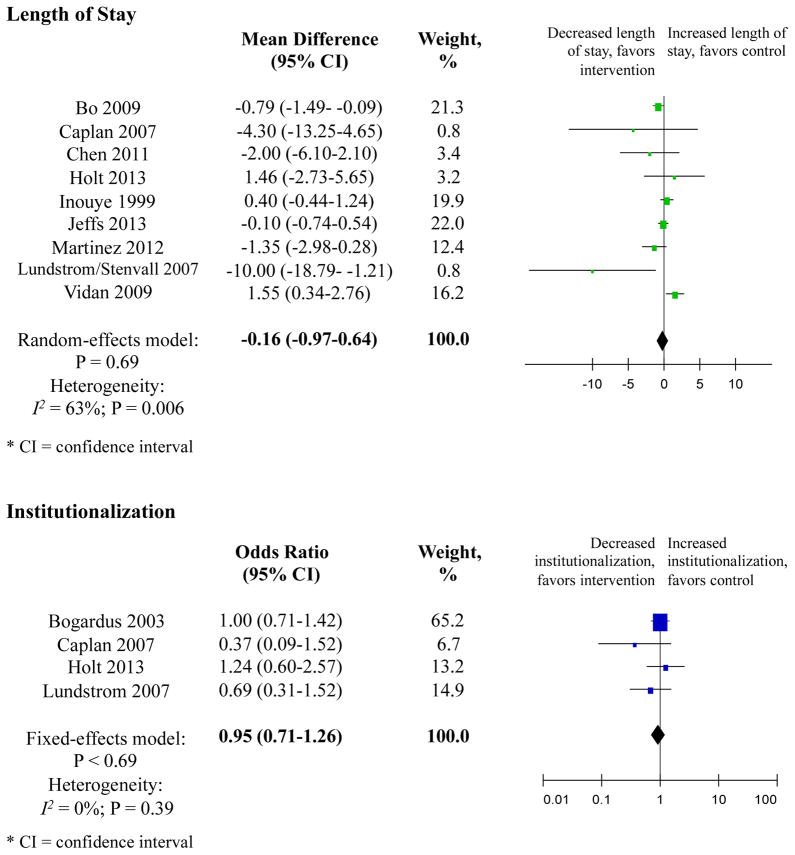
Main outcomes and measures: We identified 14 interventional studies. The results for outcomes of delirium incidence, falls, length of stay, and institutionalization were pooled for the meta-analysis, but heterogeneity limited our meta-analysis of the results for change in functional or cognitive status. Overall, 11 studies demonstrated significant reductions in delirium incidence (odds ratio [OR], 0.47; 95% CI, 0.38-0.58). Four randomized or matched trials reduced delirium incidence by 44% (OR, 0.56; 95% CI, 0.42-0.76). The rate of falls decreased significantly among intervention patients in 4 studies (OR, 0.38; 95% CI, 0.25-0.60); in 2 randomized or matched trials, the rate of falls was reduced by 64% (OR, 0.36; 95% CI, 0.22-0.61). Length of stay and institutionalization also trended toward decreases in the intervention groups, with a mean difference of -0.16 (95% CI, -0.97 to 0.64) day shorter and the odds of institutionalization 5% lower (OR, 0.95; 95% CI, 0.71-1.26). Among higher-quality randomized or matched trials, length of stay trended -0.33 (95% CI, -1.38 to 0.72) day shorter, and the odds of institutionalization trended 6% lower (OR, 0.94; 95% CI, 0.69-1.30).
Conclusions and relevance: Multicomponent nonpharmacological delirium prevention interventions are effective in reducing delirium incidence and preventing falls, with a trend toward decreasing length of stay and avoiding institutionalization. Given the current focus on prevention of hospital-based complications and improved cost-effectiveness of care, this meta-analysis supports the use of these interventions to advance acute care for older persons.
Conflict of interest statement
Figures
Comment in
-
Delirium and the "know-do" gap in acute care for elders.JAMA Intern Med. 2015 Apr;175(4):521-2. doi: 10.1001/jamainternmed.2014.7786. JAMA Intern Med. 2015. PMID: 25642659 No abstract available.
-
ACP Journal Club. Review: Multicomponent nonpharmacologic interventions reduce incident delirium in inpatients.Ann Intern Med. 2015 Jul 21;163(2):JC4. doi: 10.7326/ACPJC-2015-163-2-004. Ann Intern Med. 2015. PMID: 26192584 No abstract available.
References
-
- Witlox J, Eurelings LS, de Jonghe JF, Kalisvaart KJ, Eikelenboom P, van Gool WA. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010;304(4):443–51. - PubMed
-
- Inouye SK, Bogardus ST, Jr, Charpentier PA, Leo-Summers L, Acampora D, Holford TR, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
