

Plasma soluble thrombomodulin levels are associated with mortality in the acute respiratory distress syndrome
- PMID: 25643902
- PMCID: PMC4500527
- DOI: 10.1007/s00134-015-3648-x
Plasma soluble thrombomodulin levels are associated with mortality in the acute respiratory distress syndrome
Erratum in
-
Erratum to: plasma soluble thrombomodulin levels are associated with mortality in the acute respiratory distress syndrome.Intensive Care Med. 2015 Mar;41(3):574. doi: 10.1007/s00134-015-3703-7. Intensive Care Med. 2015. PMID: 25708422 No abstract available.
Abstract
Objective: Thombomodulin (TM) is an activator of protein C and a biomarker for endothelial injury. We hypothesized that (1) elevated plasma levels would be associated with clinical outcomes and (2) polymorphisms in the TM gene would be associated with plasma levels.
Patients: We studied 449 patients enrolled in the Fluid and Catheter Treatment Trial (FACTT) for whom both plasma and DNA were available. We used logistic regression and receiver operator curves (ROC) to test for associations between soluble TM (sTM) and mortality at 60 days.
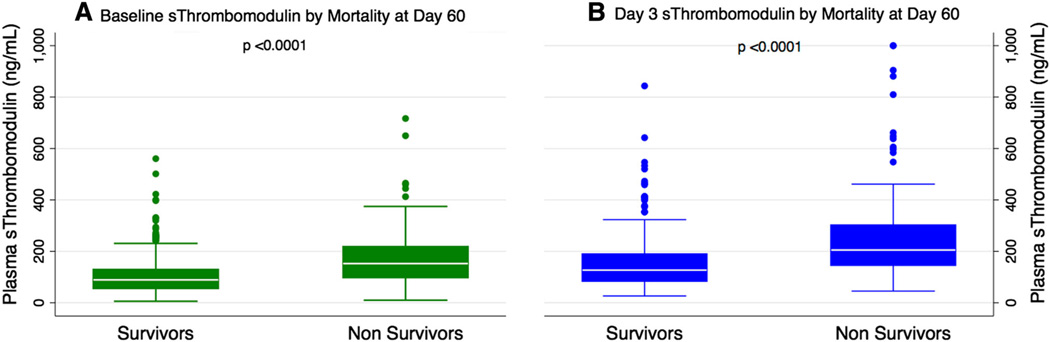
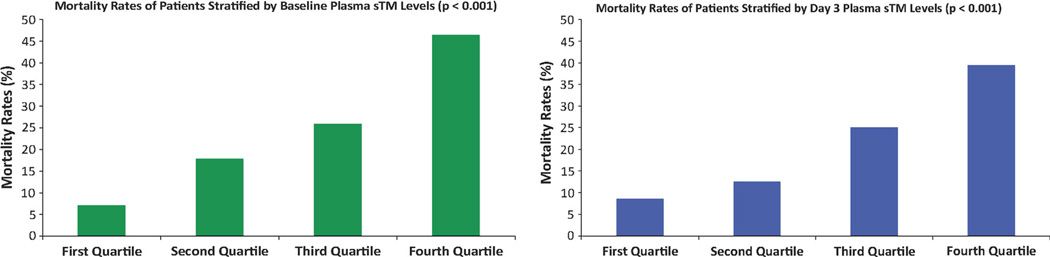
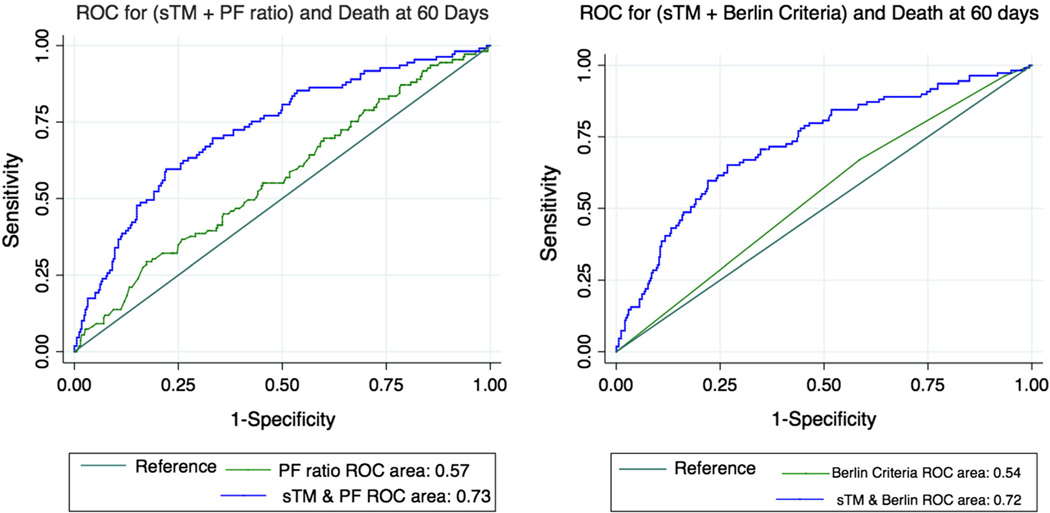
Measurements and results: Plasma sTM levels were higher in non-survivors than survivors at baseline [median 147 (IQR, 95-218) vs. 89 (56-129) ng/mL, p < 0.0001] and on day 3 after study enrollment [205 (146-302) vs. 127 (85-189), p < 0.0001]. The odds of death increased by 2.4 (95 % CI 1.5-3.8, p < 0.001), and by 2.8 (1.7-4.7, P < 0.001) for every log increase in baseline and day 3 sTM levels, respectively, after adjustment for age, race, gender, severity of illness, fluid management strategy, baseline creatinine, and non-pulmonary sepsis as the primary cause of ARDS. By ROC analysis, plasma sTM levels discriminated between non-survivors and survivors [AUC = 72 % (66-78 %) vs. AUC = 54 % for severity based on Berlin criteria). Addition of sTM improved discrimination based on APACHE III from 77 to 80 % (P < 0.03). sTM levels at baseline were not statistically different among subjects stratified by genotypes of tag SNPs in the TM gene.
Conclusions: Higher plasma sTM levels are associated with increased mortality in ARDS. The lack of association between the sTM levels and genetic variants suggests that the increased levels of sTM may reflect severity of endothelial damage rather than genetic heterogeneity. These findings underscore the importance of endothelial injury in ARDS pathogenesis and suggest that, in combination with clinical markers, sTM could contribute to risk stratification.
Conflict of interest statement
Figures
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, Stern EJ, Hudson LD. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–1693. - PubMed
-
- Zimmerman JJ, Akhtar SR, Caldwell E, Rubenfeld GD. Incidence and outcomes of pediatric acute lung injury. Pediatrics. 2009;124:87–95. - PubMed
-
- Khadaroo RG, Marshall JC. ARDS and the multiple organ dysfunction syndrome. Common mechanisms of a common systemic process. Crit Care Clin. 2002;18:127–141. - PubMed
-
- Boffa MC, Karmochkine M. Thrombomodulin: an overview and potential implications in vascular disorders. Lupus. 1998;7(Suppl 2):S120–S125. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL103836/HL/NHLBI NIH HHS/United States
- HL51856/HL/NHLBI NIH HHS/United States
- N01-HR-16146-54/HR/NHLBI NIH HHS/United States
- N01 HR016146/HR/NHLBI NIH HHS/United States
- HL110969/HL/NHLBI NIH HHS/United States
- K23 HL085526/HL/NHLBI NIH HHS/United States
- R01 HL051856/HL/NHLBI NIH HHS/United States
- K24 HL103836/HL/NHLBI NIH HHS/United States
- R37 HL051856/HL/NHLBI NIH HHS/United States
- N01-HR-46046-64/HR/NHLBI NIH HHS/United States
- K23 HL116800/HL/NHLBI NIH HHS/United States
- R21 HL112656/HL/NHLBI NIH HHS/United States
- R01 HL110969/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
