

Systematic review and meta-analysis of the performance of clinical risk assessment instruments for screening for osteoporosis or low bone density
- PMID: 25644147
- PMCID: PMC4401628
- DOI: 10.1007/s00198-015-3025-1
Systematic review and meta-analysis of the performance of clinical risk assessment instruments for screening for osteoporosis or low bone density
Abstract
We performed a systematic review and meta-analysis of the performance of clinical risk assessment instruments for screening for DXA-determined osteoporosis or low bone density. Commonly evaluated risk instruments showed high sensitivity approaching or exceeding 90% at particular thresholds within various populations but low specificity at thresholds required for high sensitivity. Simpler instruments, such as OST, generally performed as well as or better than more complex instruments.
Introduction: The purpose of the study is to systematically review the performance of clinical risk assessment instruments for screening for dual-energy X-ray absorptiometry (DXA)-determined osteoporosis or low bone density.
Methods: Systematic review and meta-analysis were performed. Multiple literature sources were searched, and data extracted and analyzed from included references.
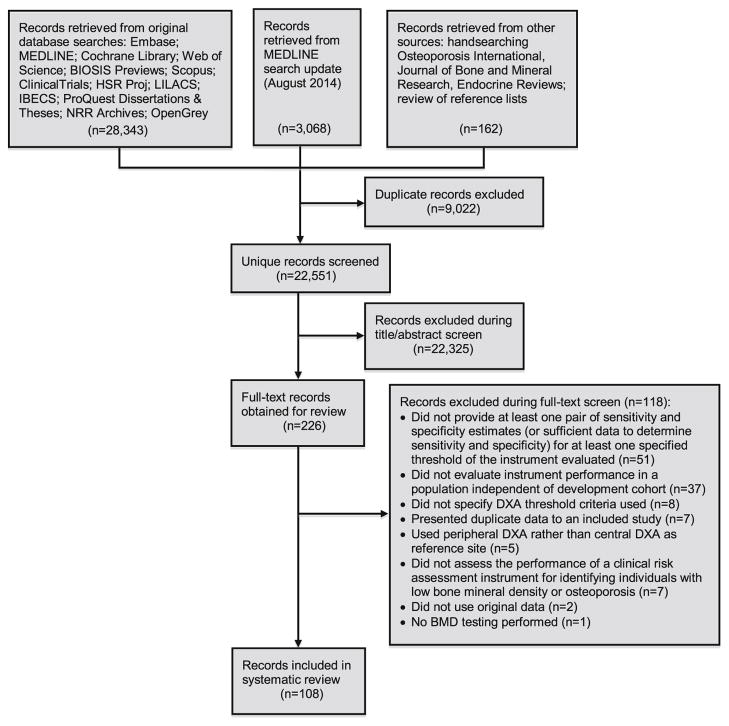
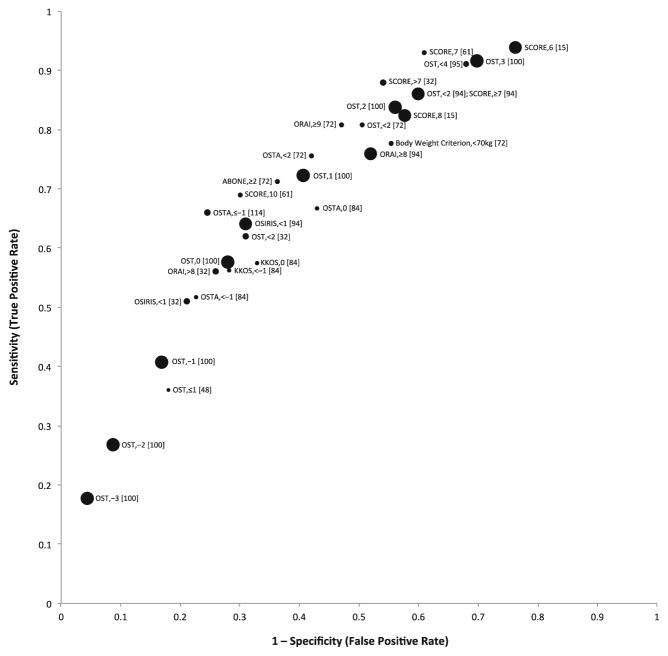
Results: One hundred eight references met inclusion criteria. Studies assessed many instruments in 34 countries, most commonly the Osteoporosis Self-Assessment Tool (OST), the Simple Calculated Osteoporosis Risk Estimation (SCORE) instrument, the Osteoporosis Self-Assessment Tool for Asians (OSTA), the Osteoporosis Risk Assessment Instrument (ORAI), and body weight criteria. Meta-analyses of studies evaluating OST using a cutoff threshold of <1 to identify US postmenopausal women with osteoporosis at the femoral neck provided summary sensitivity and specificity estimates of 89% (95%CI 82-96%) and 41% (95%CI 23-59%), respectively. Meta-analyses of studies evaluating OST using a cutoff threshold of 3 to identify US men with osteoporosis at the femoral neck, total hip, or lumbar spine provided summary sensitivity and specificity estimates of 88% (95%CI 79-97%) and 55% (95%CI 42-68%), respectively. Frequently evaluated instruments each had thresholds and populations for which sensitivity for osteoporosis or low bone mass detection approached or exceeded 90% but always with a trade-off of relatively low specificity.
Conclusions: Commonly evaluated clinical risk assessment instruments each showed high sensitivity approaching or exceeding 90% for identifying individuals with DXA-determined osteoporosis or low BMD at certain thresholds in different populations but low specificity at thresholds required for high sensitivity. Simpler instruments, such as OST, generally performed as well as or better than more complex instruments.
Conflict of interest statement
Figures
References
-
- Lin JT, Lane JM. Osteoporosis: a review. Clin Orthop Relat Res. 2004:126–134. - PubMed
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22:465–475. - PubMed
-
- U.S. Department of Health and Human Services. Bone health and osteoporosis: a report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, Office of the Surgeon General; 2004.
-
- Stafford RS, Drieling RL, Hersh AL. National trends in osteoporosis visits and osteoporosis treatment, 1988–2003. Arch Intern Med. 2004;164:1525–1530. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
