

Emergency surgery in the elderly: the balance between function, frailty, fatality and futility
- PMID: 25645443
- PMCID: PMC4320594
- DOI: 10.1186/s13049-015-0099-x
Emergency surgery in the elderly: the balance between function, frailty, fatality and futility
Abstract
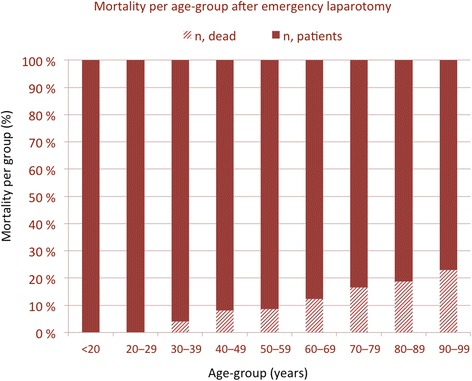
Becoming old is considered a privilege and results from the socioeconomic progress and improvements in health care systems worldwide. However, morbidity and mortality increases with age, and even more so in acute onset disease. With the current prospects of longevity, a considerable number of elderly patients will continue to live with good function and excellent quality of life after emergency surgical care. However, mortality in emergency surgery may be reported at 15-30%, doubled if associated with complications, and notably higher in patients over 75 years. A number of risks associated with death are reported, and a number of scores proposed for prediction of risk. Frailty, a decline in the physiological reserves that may make the person vulnerable to even the most minor of stressful event, appears to be a valid indicator and predictor of risk and poor outcome, but how to best address and measure frailty in the emergency setting is not clear. Futility may sometimes be clearly defined, but most often becomes a borderline decision between ethics, clinical predictions and patient communication for which no solid evidence currently exists. The number and severity of other underlying condition(s), as well as the treatment alternatives and their consequences, is a complex picture to interpret. Add in the onset of the acute surgical disease as a further potential detrimental factor on function and quality of life - and you have a perfect storm to handle. In this brief review, some of the challenging aspects related to emergency surgery in the elderly will be discussed. More research, including registries and trials, are needed for improved knowledge to a growing health care challenge.
Figures
References
-
- Ageing well: a global priority. Lancet 2012;379(9823):1274. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
