

The effect of clopidogrel on platelet activity in patients with and without type-2 diabetes mellitus: a comparative study
- PMID: 25645908
- PMCID: PMC4324649
- DOI: 10.1186/s12933-015-0182-7
The effect of clopidogrel on platelet activity in patients with and without type-2 diabetes mellitus: a comparative study
Abstract
Background: Although antiplatelet therapy involving clopidogrel is a standard treatment for preventing cardiovascular events after coronary stent implantation, patients can display differential responses. Here, we assessed the effectiveness of clopidogrel on platelet function inhibition in subjects with and without type-2 diabetes and stable coronary artery disease. In addition, we investigated the correlation between platelet function and routine clinical parameters.
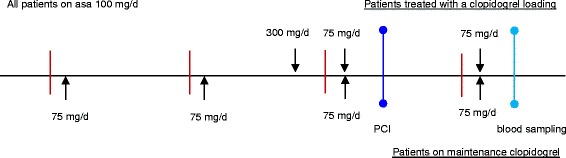
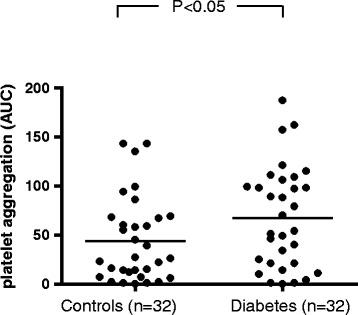
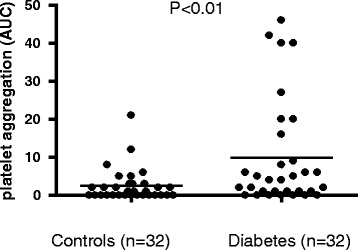
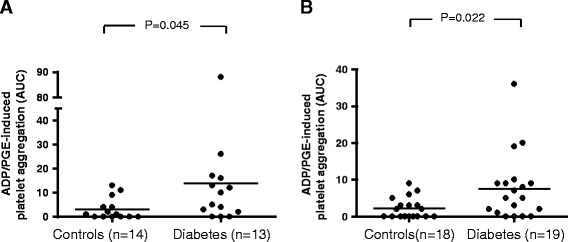
Methods: A total of 64 patients with stable coronary heart disease were enrolled in the study. Among these, 32 had known type-2 diabetes, whereas the remaining 32 subjects were non-diabetics (control group). A loading dose of 300 mg clopidogrel was given to clopidogrel-naïve patients (13 patients in the diabetes group and 14 control patients). All patients were given a daily maintenance dose of 75 mg clopidogrel. In addition, all patients received 100 mg ASA per day. Agonist-induced platelet aggregation measurements were performed on hirudin-anticoagulated blood using an impedance aggregometer (Multiple Platelet Function Analyzer, Dynabyte, Munich, Germany). Blood samples were drawn from the antecubital vein 24 h after coronary angiography with percutaneous coronary intervention. The platelets were then stimulated with ADP alone or ADP and prostaglandin-E (ADP and ADP-PGE tests, respectively) in order to evaluate clopidogrel-mediated inhibition of platelet function. The effectiveness of ASA was measured by stimulation with arachidonic acid (ASPI test). In addition, maximal platelet aggregation was assessed via stimulation with thrombin receptor-activating peptide (TRAP test).
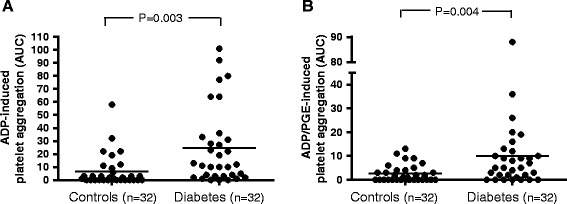
Results: Patients with diabetes exhibited significantly less inhibition of platelet function than patients without diabetes (ADP-PGE test p = 0.003; ASPI test p = 0.022). Administering a clopidogrel loading dose of 300 mg did not result in a lower level of ADP-PGE-induced platelet reactivity in comparison to the use of a 75 mg maintenance dose. Moreover, we observed that ADP-PGE-induced platelet inhibition was positively correlated with fasting blood glucose and HbA1c (p < 0.01).
Conclusions: Patients with type-2 diabetes exhibited increased platelet reactivity compared to patients without diabetes despite combined treatment with clopidogrel and ASA. Using a loading dose of clopidogrel rather than small daily doses was not sufficient for adequately overcoming increased platelet reactivity in patients with type-2 diabetes, highlighting the need for more effective anti-platelet drugs for such patients.
Figures
Similar articles
-
Vitamin D levels and high-residual platelet reactivity in patients receiving dual antiplatelet therapy with clopidogrel or ticagrelor.Platelets. 2016 Sep;27(6):576-82. doi: 10.3109/09537104.2016.1149159. Epub 2016 Apr 11. Platelets. 2016. PMID: 27540959
-
Postmenopausal women have an increased maximal platelet reactivity compared to men despite dual antiplatelet therapy.Blood Coagul Fibrinolysis. 2012 Dec;23(8):723-8. doi: 10.1097/MBC.0b013e32835824b3. Blood Coagul Fibrinolysis. 2012. PMID: 23135379
-
Platelet reactivity in patients with impaired renal function receiving dual antiplatelet therapy with clopidogrel or ticagrelor.Vascul Pharmacol. 2016 Apr;79:11-15. doi: 10.1016/j.vph.2015.10.006. Epub 2015 Oct 28. Vascul Pharmacol. 2016. PMID: 26518440
-
Does percutaneous coronary stent implantation increase platelet reactivity?Blood Rev. 2017 Sep;31(5):271-275. doi: 10.1016/j.blre.2017.03.003. Epub 2017 Mar 8. Blood Rev. 2017. PMID: 28302342 Review.
-
Challenges and perspectives of antiplatelet therapy in patients with diabetes mellitus and coronary artery disease.Curr Pharm Des. 2012;18(33):5273-93. doi: 10.2174/138161212803251916. Curr Pharm Des. 2012. PMID: 22724415 Review.
Cited by
-
Combined impact of body mass index and glycemic control on the efficacy of clopidogrel-aspirin therapy in patients with minor stroke or transient ischemic attack.Aging (Albany NY). 2020 Jun 16;12(12):12175-12186. doi: 10.18632/aging.103394. Epub 2020 Jun 16. Aging (Albany NY). 2020. PMID: 32544082 Free PMC article. Clinical Trial.
-
Ticagrelor and prasugrel are independent predictors of improved long-term survival in ACS patients.Eur J Clin Invest. 2020 Nov;50(11):e13304. doi: 10.1111/eci.13304. Epub 2020 Sep 9. Eur J Clin Invest. 2020. PMID: 32506444 Free PMC article.
-
Association between insulin receptor substrate-1 polymorphisms and high platelet reactivity with clopidogrel therapy in coronary artery disease patients with type 2 diabetes mellitus.Cardiovasc Diabetol. 2016 Mar 22;15:50. doi: 10.1186/s12933-016-0362-0. Cardiovasc Diabetol. 2016. PMID: 27005817 Free PMC article. Clinical Trial.
-
Chronic Inflammatory Status Observed in Patients with Type 2 Diabetes Induces Modulation of Cytochrome P450 Expression and Activity.Int J Mol Sci. 2021 May 7;22(9):4967. doi: 10.3390/ijms22094967. Int J Mol Sci. 2021. PMID: 34067027 Free PMC article. Review.
-
Poor glycaemic control contributes to a shift towards prothrombotic and antifibrinolytic state in pregnant women with type 1 diabetes mellitus.PLoS One. 2020 Oct 8;15(10):e0237843. doi: 10.1371/journal.pone.0237843. eCollection 2020. PLoS One. 2020. PMID: 33031385 Free PMC article.
References
-
- Chesebro JH, Rauch U, Fuster V, Badimon JJ. Pathogenesis of thrombosis in coronary artery disease. Haemostasis. 1997;27:12–8. - PubMed
-
- Steinhubl SR, Berger PB, Mann JT, III, Fry ET, DeLago A, Wilmer C, et al. CREDO Investigators. Clopidogrel for the reduction of events during observation. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288:2411–20. doi: 10.1001/jama.288.19.2411. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
