

Diagnostic accuracy of single baseline measurement of Elecsys Troponin T high-sensitive assay for diagnosis of acute myocardial infarction in emergency department: systematic review and meta-analysis
- PMID: 25646632
- PMCID: PMC4300724
- DOI: 10.1136/bmj.h15
Diagnostic accuracy of single baseline measurement of Elecsys Troponin T high-sensitive assay for diagnosis of acute myocardial infarction in emergency department: systematic review and meta-analysis
Abstract
Objective: To obtain summary estimates of the accuracy of a single baseline measurement of the Elecsys Troponin T high-sensitive assay (Roche Diagnostics) for the diagnosis of acute myocardial infarction in patients presenting to the emergency department.
Design: Systematic review and meta-analysis of diagnostic test accuracy studies.
Data sources: Medline, Embase, and other relevant electronic databases were searched for papers published between January 2006 and December 2013.
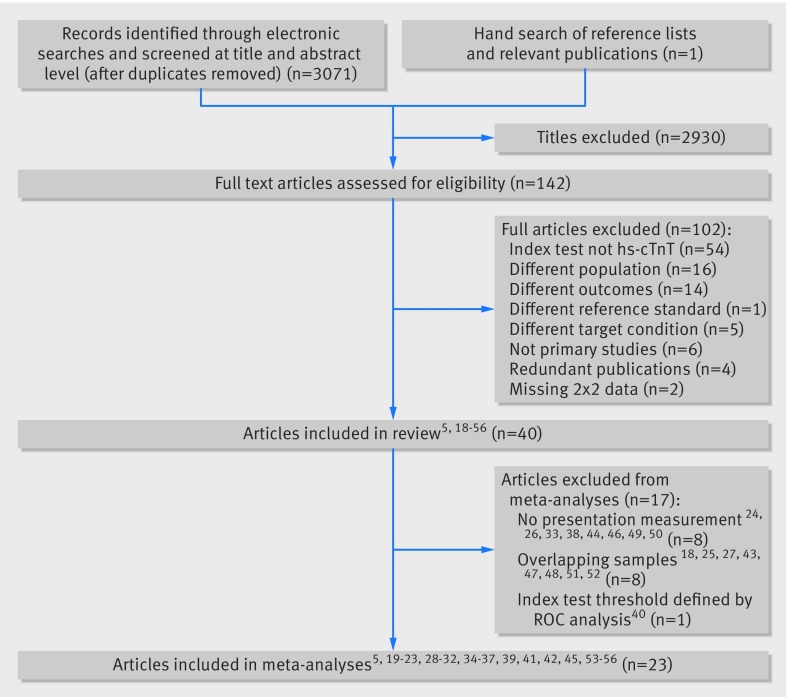
Study selection: Studies were included if they evaluated the diagnostic accuracy of a single baseline measurement of Elecsys Troponin T high-sensitive assay for the diagnosis of acute myocardial infarction in patients presenting to the emergency department with suspected acute coronary syndrome.
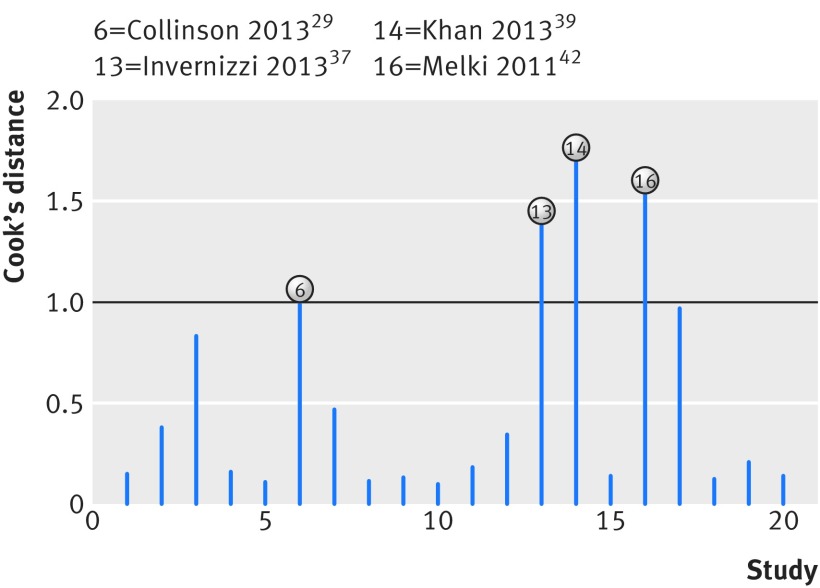
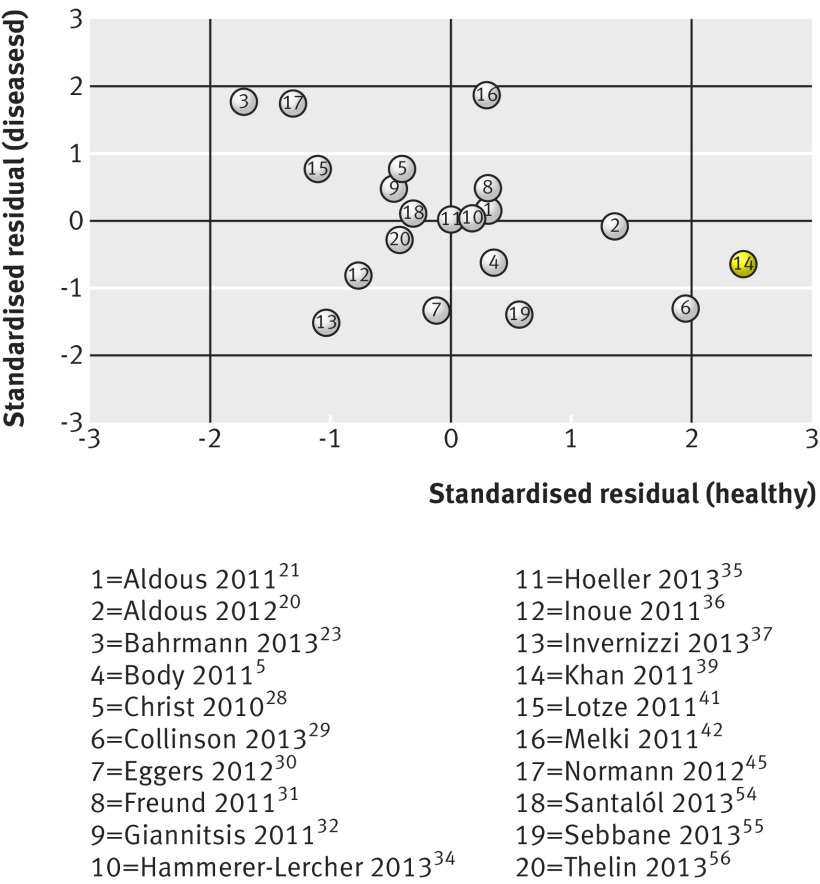
Study appraisal and data synthesis: The first author screened all titles and abstracts identified through the searches and selected all potentially relevant papers. The screening of the full texts, the data extraction, and the methodological quality assessment, using the adapted QUADAS-2 tool, were conducted independently by two reviewers with disagreements being resolved through discussion or arbitration. If appropriate, meta-analysis was conducted using the hierarchical bivariate model.
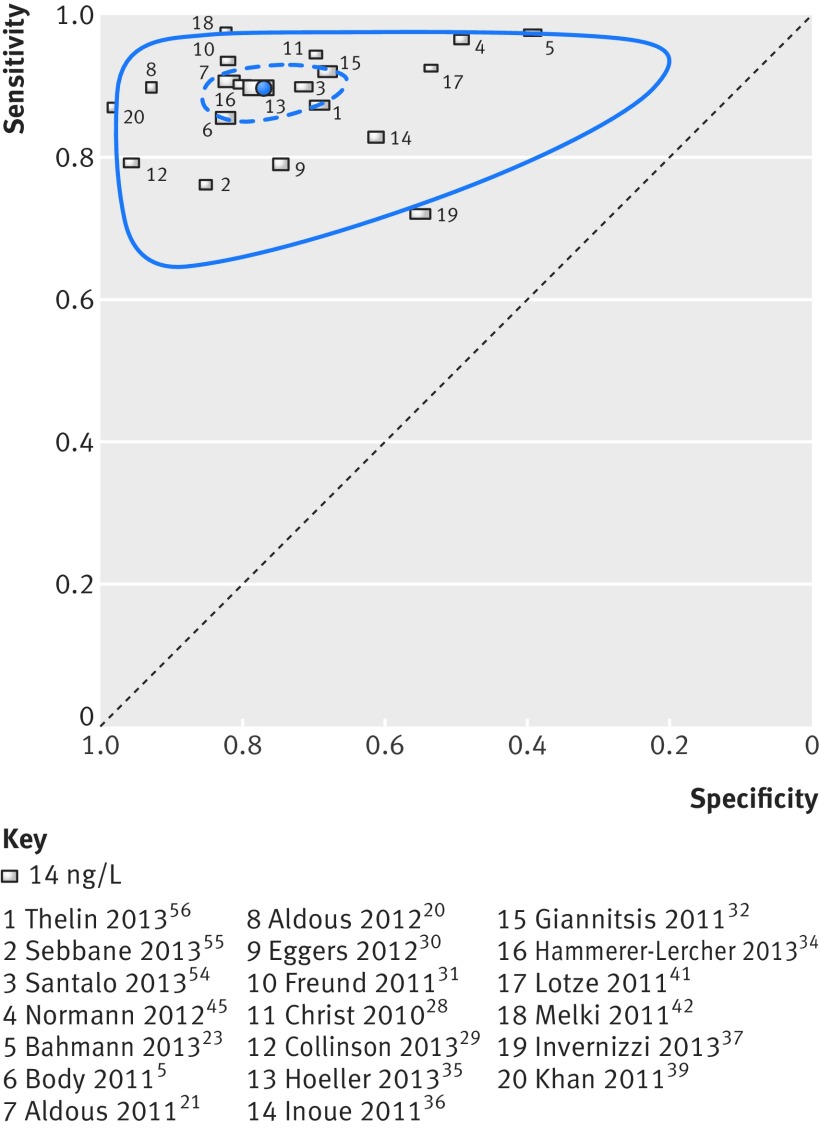
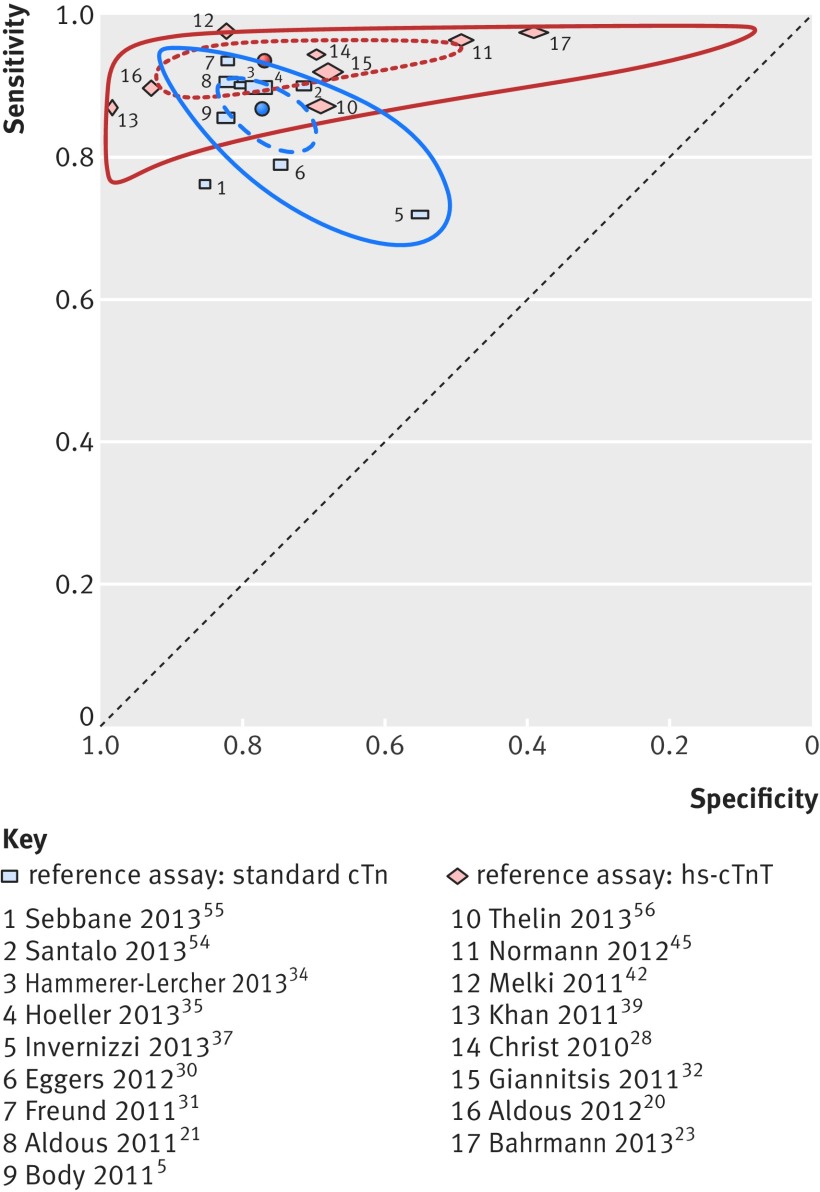
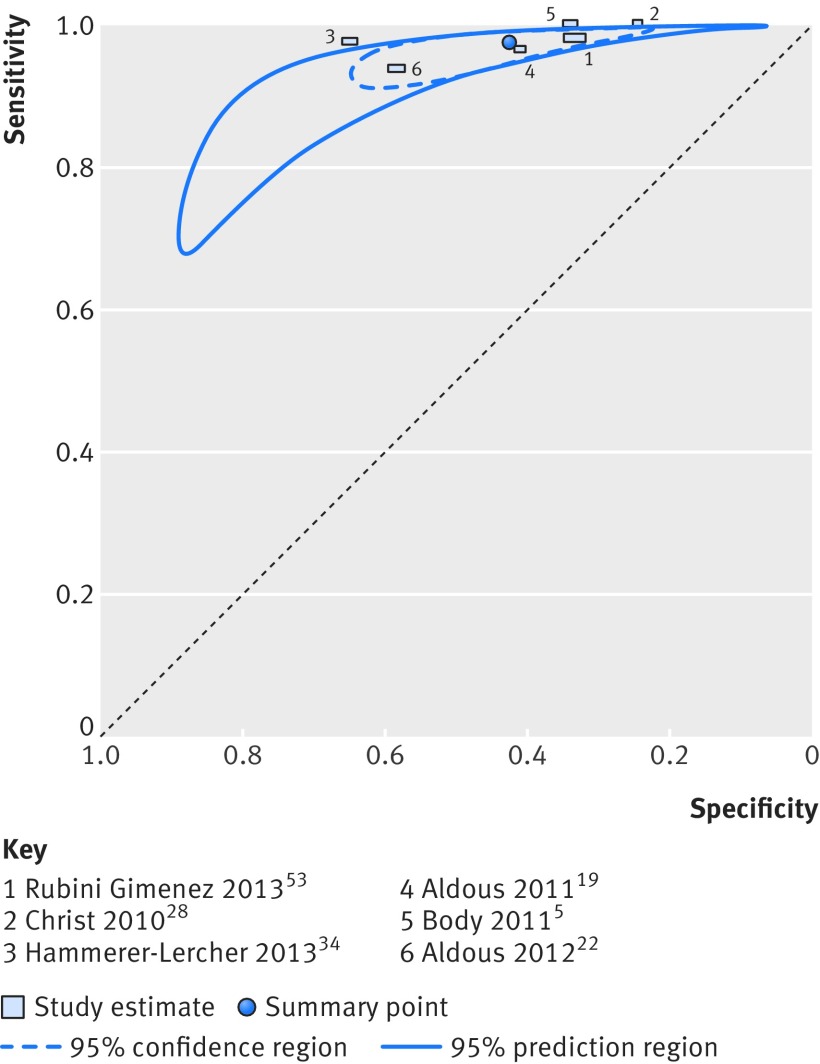
Results: Twenty three studies reported the performance of the evaluated assay at presentation. The results for 14 ng/L and 3-5 ng/L cut-off values were pooled separately. At 14 ng/L (20 papers), the summary sensitivity was 89.5% (95% confidence interval 86.3% to 92.1%) and the summary specificity was 77.1% (68.7% to 83.7%). At 3-5 ng/L (six papers), the summary sensitivity was 97.4% (94.9% to 98.7%) and the summary specificity was 42.4% (31.2% to 54.5%). This means that if 21 of 100 consecutive patients have the target condition (21%, the median prevalence across the studies), 2 (95% confidence interval 2 to 3) of 21 patients with acute myocardial infarction will be missed (false negatives) if 14 ng/L is used as a cut-off value and 18 (13 to 25) of 79 patients without acute myocardial infarction will test positive (false positives). If the 3-5 ng/L cut-off value is used, <1 (0 to 1) patient with acute myocardial infarction will be missed and 46 (36 to 54) patients without acute myocardial infarction will test positive.
Conclusions: The results indicate that a single baseline measurement of the Elecsys Troponin T high-sensitive assay could be used to rule out acute myocardial infarction if lower cut-off values such as 3 ng/L or 5 ng/L are used. However, this method should be part of a comprehensive triage strategy and may not be appropriate for patients who present less than three hours after symptom onset. Care must also be exercised because of the higher imprecision of the evaluated assay and the greater effect of lot-to-lot reagent variation at low troponin concentrations.
Systematic review registration: PROSPERO registration number CRD42013003926.
© Zhelev et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures


Comment in
-
Biomarkers: High-sensitivity troponin assays for the diagnosis of AMI-sex-specific differences?Nat Rev Cardiol. 2015 Mar;12(3):129. doi: 10.1038/nrcardio.2015.15. Epub 2015 Feb 10. Nat Rev Cardiol. 2015. PMID: 25666408 No abstract available.
-
Is a Single High-Sensitivity Troponin T Assay Accurate for the Detection of Acute Myocardial Infarction?Ann Emerg Med. 2016 Sep;68(3):295-7. doi: 10.1016/j.annemergmed.2016.02.046. Epub 2016 Apr 13. Ann Emerg Med. 2016. PMID: 27083856 No abstract available.
References
-
- Niska R, Bhuiya F, Xu J. National hospital ambulatory medical care survey: 2007 emergency department summary. Natl Health Stat Report 2010;26:1-31. - PubMed
-
- Hamm CW, Bassand J-P, Agewall S, Bax J, Boersma E, Bueno H, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2011;32:2999-3054. - PubMed
-
- Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med 2000;342:1163-70. - PubMed
-
- Body R, Carley S, McDowell G, Jaffe AS, France M, Cruickshank K, et al. Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol 2011;58:1332-9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous