

Trauma-informed medical care: CME communication training for primary care providers
- PMID: 25646872
- PMCID: PMC4316735
Trauma-informed medical care: CME communication training for primary care providers
Abstract
Background and objectives: Trauma exposure predicts mental disorders, medical morbidity, and health care costs. Yet trauma-related impacts have not received sufficient attention in primary care provider (PCP) training programs. This study adapted a theory-based approach to working with trauma survivors, Risking Connection, into a 6-hour CME course, Trauma-Informed Medical Care (TI-Med), and evaluated its efficacy.
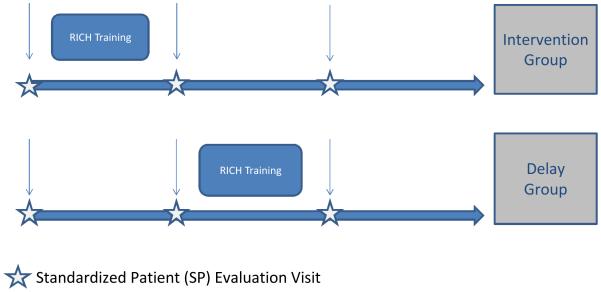
Methods: We randomized PCPs to training or wait-list (delay) conditions; wait-list groups were trained after reassessment. The primary outcome assessing newly acquired skills was a patient-centeredness score derived from Roter Interactional Analysis System ratings of 90 taped visits between PCPs and standardized patients (SPs). PCPs were family medicine residents (n=17) and community physicians (n=13, 83% family medicine specialty), from four sites in the Washington, DC metropolitan area.
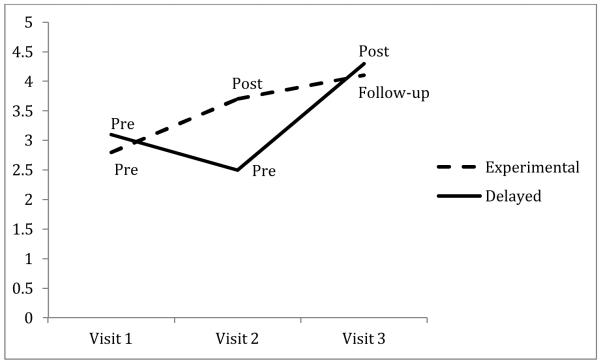
Results: Immediately trained PCPs trended toward a larger increase in patient centeredness than did the delayed PCPs, with a moderate effect size (.66). The combined trained PCP groups showed a significant increase in patient centeredness from before to after training.
Conclusions: This is a promising approach to supporting relationship-based trauma-informed care among PCPs to help promote better patient health and higher compliance with medical treatment plans.
Figures
References
-
- Breslau N. Gender differences in trauma and posttraumatic stress disorder. J Gend Specif Med. 2002;5(1):34–40. - PubMed
-
- Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the national comorbidity survey. Arch Gen Psychiatry. 1995;52(12):1048–1060. - PubMed
-
- Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. 1998;14(4):245–258. - PubMed
-
- Green BL. Psychosocial research in traumatic stress: An update. J Trauma Stress. 1994;7(3):341–362. - PubMed
-
- Roth S, Newman E, Pelcovitz D, van der Kolk B, Mandel FS. Complex PTSD in victims exposed to sexual and physical abuse: Results from the DSM-IV field trial for posttraumatic stress disorder. J Trauma Stress. 1997;10(4):539–555. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
