

Comprehensive evaluation of the immune risk phenotype in successfully treated HIV-infected individuals
- PMID: 25647167
- PMCID: PMC4315523
- DOI: 10.1371/journal.pone.0117039
Comprehensive evaluation of the immune risk phenotype in successfully treated HIV-infected individuals
Abstract
Background: Despite successful treatment and CD4+ T-cell recovery, HIV-infected individuals often experience a profound immune dysregulation characterized by a persistently low CD4:CD8 T-cell ratio. This residual immune dysregulation is reminiscent of the Immune Risk Phenotype (IRP) previously associated with morbidity and mortality in the uninfected elderly (>85 years). The IRP consists of laboratory markers that include: a low CD4:CD8 T-cell ratio, an expansion of CD8+CD28- T-cells and cytomegalovirus (CMV) seropositivity. Despite the significant overlap in immunological phenotypes between normal aging and HIV infection, the IRP has never been evaluated in HIV-infected individuals. In this pilot study we characterized immune changes associated with the IRP in a sample of successfully treated HIV-infected subjects.
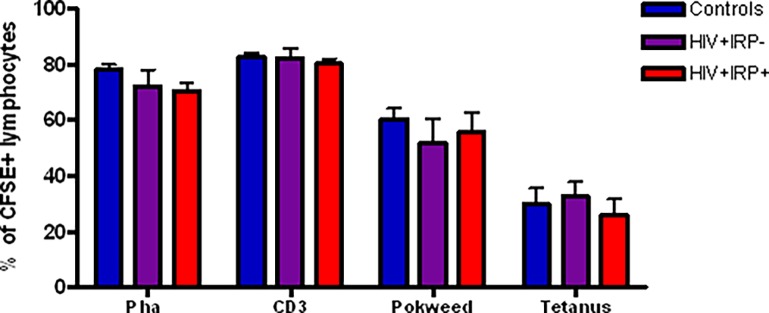
Methods: 18 virologically suppressed HIV-infected subjects were categorized into 2 groups based on their IRP status; HIV+IRP+, (n = 8) and HIV+IRP-, (n = 10) and compared to 15 age-matched HIV uninfected IRP negative controls. All individuals were assessed for functional and phenotypic immune characteristics including: pro-inflammatory cytokine production, antigen-specific proliferation capacity, replicative senescence, T-cell differentiation and lymphocyte telomere length.
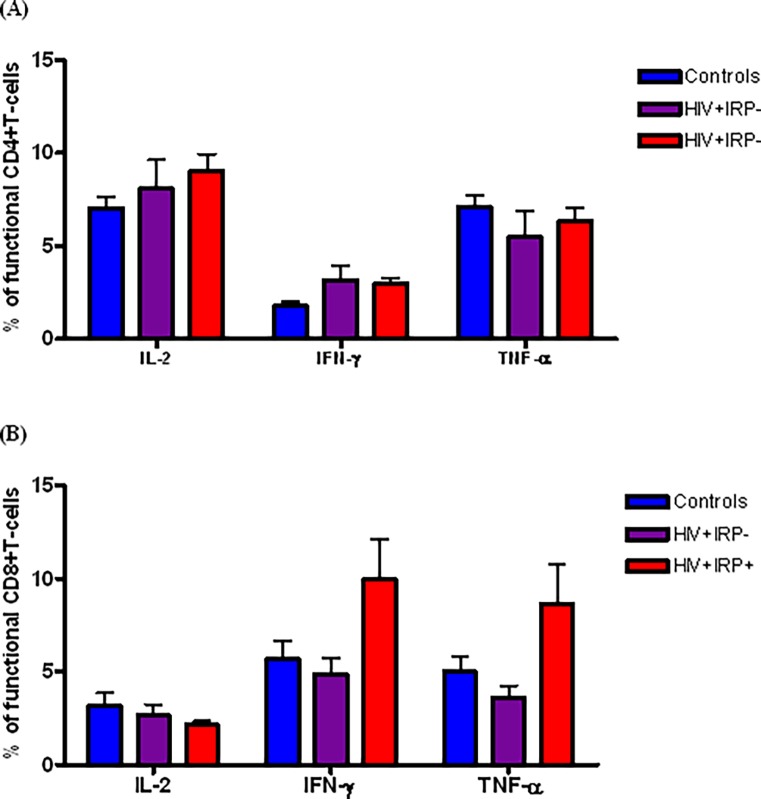
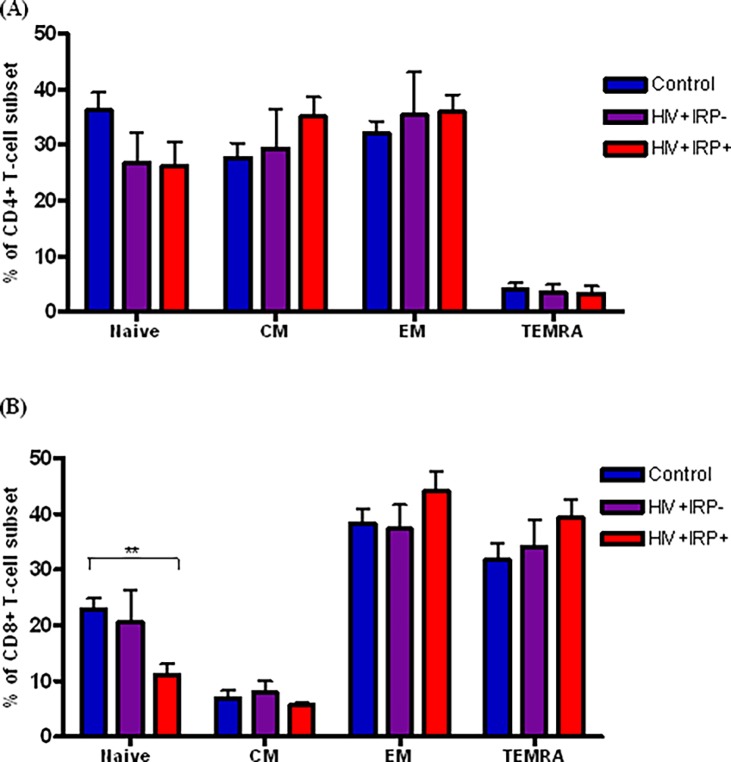
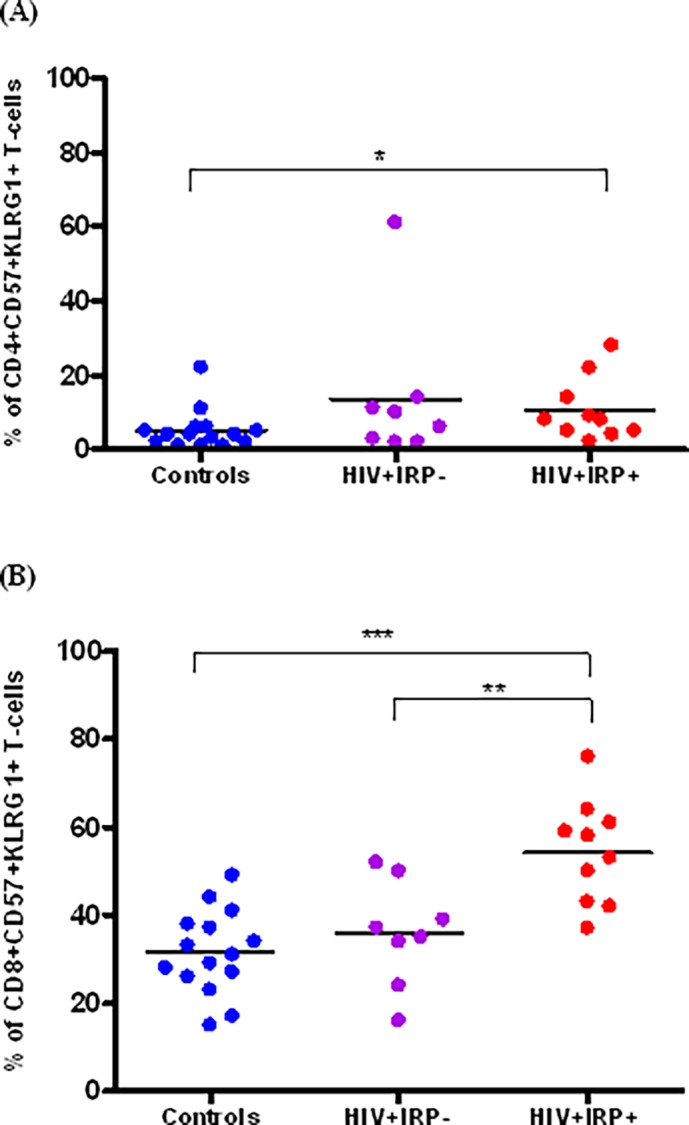
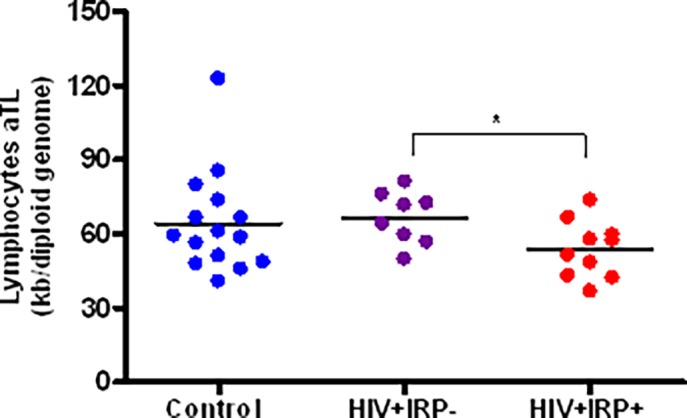
Results: Compared to HIV-infected subjects without an IRP, HIV+IRP+ subjects exhibited a higher frequency of TNF-α-producing CD8+ T-cells (p = 0.05) and a reduced proportion of CD8+ naïve T-cells (p = 0.007). The IRP status was also associated with a marked up-regulation of the replicative senescence markers CD57 and KLGR1, on the surface of CD8+T-cells (p = 0.004). Finally, HIV+IRP+ individuals had a significantly shorter mean lymphocyte telomere length than their non-IRP counterparts (p = 0.03).
Conclusions: Our findings suggest that, despite similar levels of treatment-mediated viral suppression, the phenotypic and functional immune characteristics of HIV+IRP+ individuals are distinct from those observed in non-IRP individuals. The IRP appears to identify a subset of treated HIV-infected individuals with a higher degree of immune senescence.
Conflict of interest statement
Figures
References
-
- Gottlieb MS, Schroff R, Schanker HM, Weisman JD, Fan PT, et al. (1981) Pneumocystis carinii pneumonia and mucosal candidiasis in previously healthy homosexual men: evidence of a new acquired cellular immunodeficiency. N Engl J Med 305: 1425–1431. - PubMed
-
- Moore RD, Keruly JC (2007) CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin Infect Dis 44: 441–446. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
