

Inoperable inflammatory myofibroblastic tumour of the para-nasal sinuses and orbit with recurrence responding to methotrexate and prednisolone: a case report
- PMID: 25648655
- PMCID: PMC4323114
- DOI: 10.1186/s13104-015-0993-3
Inoperable inflammatory myofibroblastic tumour of the para-nasal sinuses and orbit with recurrence responding to methotrexate and prednisolone: a case report
Abstract
Background: Inflammatory myofibroblastic tumour is a rare neoplasm with a potential to behave in a malignant manner. It can occur anywhere in the body, however involvement of the head, especially the para-nasal sinuses is rare.
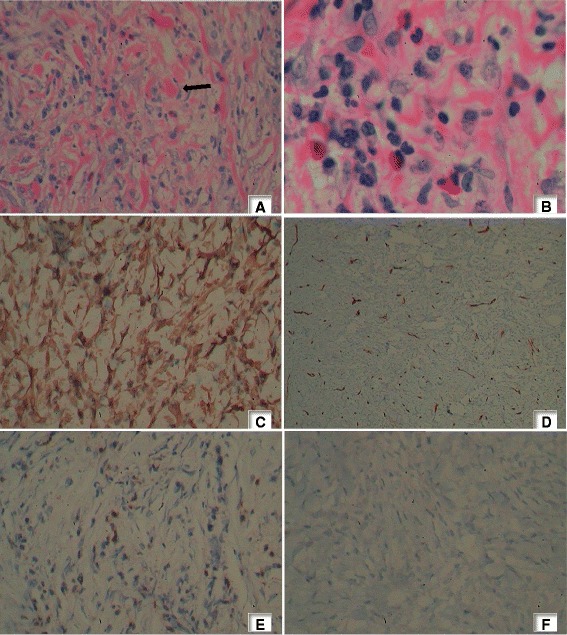
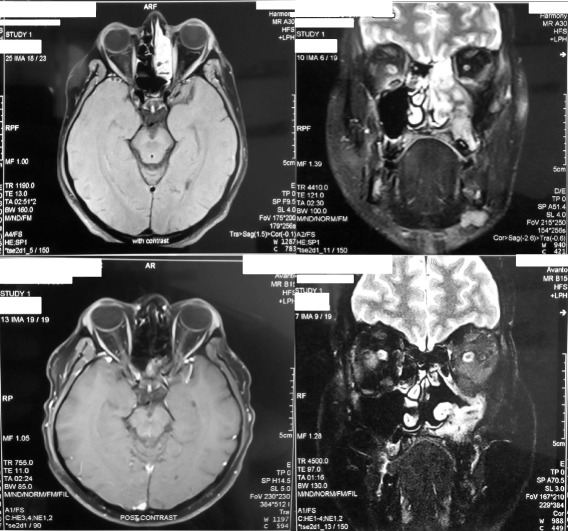
Case presentation: A 33-year-old South Asian male presented with coryzal symptoms including a persistent cough with an asymmetrical swelling of the left side of the face. Imaging revealed a mass lesion involving the para-nasal sinuses eroding into the orbit. Histology and the clinical picture were compatible with inflammatory myofibroblastic tumour. As curative excision of the tumour was not feasible, medical management was offered. Despite early features of remission to glucocorticoids, tapering resulted in recurrence. Hence combination therapy with glucocorticoids and methotrexate was commenced with dramatic reduction of tumour burden and the patient has been in remission to date.
Conclusion: Inflammatory myofibroblastic tumour has the potential to behave in a malignant manner. Medical management with chemotherapy, glucocorticoids and non-steroidal anti-inflammatory drugs though effective, do not have a uniform response pattern. Surgically unresectable inflammatory myofibroblastic tumour above neck should be treated aggressively with combination regimens. Combination of prednisolone with methotrexate has been shown to have good outcome.
Figures

Similar articles
-
[Clinical analysis of imflammatory myofibroblastic tumor of the nasal cavity and paranasal sinus].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015 Oct;29(19):1739-42. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015. PMID: 26999851 Chinese.
-
Inflammatory myofibroblastic tumour of paranasal sinuses with fatal outcome: reactive lesion or tumour?J Clin Pathol. 2003 Sep;56(9):715-7. doi: 10.1136/jcp.56.9.715. J Clin Pathol. 2003. PMID: 12944561 Free PMC article.
-
Successful treatment of an unresectable inflammatory myofibroblastic tumor of the frontal bone using a cyclooxygenase-2 inhibitor and methotrexate.Intern Med. 2013;52(5):623-8. doi: 10.2169/internalmedicine.52.8785. Epub 2013 Mar 1. Intern Med. 2013. PMID: 23448776 Review.
-
Inflammatory pseudotumour of the paranasal sinuses--a case report.Auris Nasus Larynx. 2007 Dec;34(4):533-6. doi: 10.1016/j.anl.2007.01.003. Epub 2007 Feb 28. Auris Nasus Larynx. 2007. PMID: 17331689
-
Inflammatory myofibroblastic tumors of the nasal cavity and paranasal sinus: a clinicopathologic study of 25 cases and review of the literature.Eur Arch Otorhinolaryngol. 2015 Apr;272(4):789-797. doi: 10.1007/s00405-014-3026-2. Epub 2014 Apr 23. Eur Arch Otorhinolaryngol. 2015. PMID: 24756612 Review.
Cited by
-
Inflammatory Myofibroblastic Tumour of the Bladder in a Young Male: A Rare Case Report.Cureus. 2025 May 7;17(5):e83657. doi: 10.7759/cureus.83657. eCollection 2025 May. Cureus. 2025. PMID: 40486359 Free PMC article.
-
Inflammatory Myofibroblastic Tumors in Paranasal Sinus and Nasopharynx: A Clinical Retrospective Study of 13 Cases.Biomed Res Int. 2018 Oct 15;2018:7928241. doi: 10.1155/2018/7928241. eCollection 2018. Biomed Res Int. 2018. PMID: 30410939 Free PMC article.
-
Inflammatory myofibroblastic tumor directly invading the right first rib treated with oral steroids: a case report.BMC Pulm Med. 2024 Feb 2;24(1):67. doi: 10.1186/s12890-024-02873-6. BMC Pulm Med. 2024. PMID: 38308319 Free PMC article.
-
Recurrent inflammatory myofibroblastic tumor of the inguinal region: A case report and review of the literature.Oncol Lett. 2015 Aug;10(2):675-680. doi: 10.3892/ol.2015.3297. Epub 2015 May 29. Oncol Lett. 2015. PMID: 26622552 Free PMC article.
-
Outstanding Response in a Patient With ROS1-Rearranged Inflammatory Myofibroblastic Tumor of Soft Tissues Treated With Crizotinib: Case Report.Front Oncol. 2021 Jun 15;11:658327. doi: 10.3389/fonc.2021.658327. eCollection 2021. Front Oncol. 2021. PMID: 34211840 Free PMC article.
References
-
- Zhou SH, Ruan LX, Xu YY, Wang SQ, Ren GP, Ling L. Inflammatory myofibroblastic tumour in the left maxillary sinus: a case report. Chin Med J. 2004;117(10):1597–1599. - PubMed
-
- Perez-Ordonez B, Rosai J. Follicular dendritic cell tumor: review of the entity. Semin Diagn Pathol. 1998;15(2):144–154. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
